6899-6822 Pneumonia, pneumocystis carinii
Definition
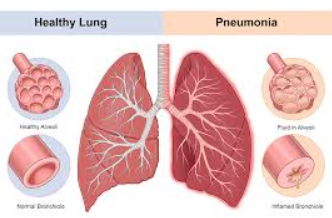
An acute interstitial plasma cell pneumonia caused by Pneumocystis carinii, an organism currently categorized as a fungus.
{kind=link}
Etiology
Infection from Pneumocystis carinii, which can reside harmlessly in normal lungs, may occur when the body's defenses are immunocompromised and weakened by disease or medications, such as cancer and cancer treatments. It is a common opportunistic infection of acquired immunodeficiency syndrome (AIDS). More than 80 percent of individuals with AIDS develop pneumocystis pneumonia when standard treatments have not been implemented. Often, pneumocystis pneumonia is the first indication that a person with human immunodeficiency virus (HIV) (see Diagnostic Code: 6351 HIV-Related illness) infection has developed AIDS.
Signs & Symptoms
{kind=link}
{kind=link}
{kind=link}
Tests
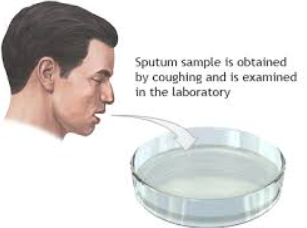
Physical examination and auscultation with a stethoscope, chest x-ray, sputum cultures, bronchoalveolar lavage, tissue biopsy, and blood studies may be valuable in diagnosing and identifying the causative organism. Computed tomography (CT) scan of the chest may be useful in complicated infections.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment
Trimethoprim-sulfamethoxazole (Bactrim) given by mouth is the usual antibiotic used in the treatment of pneumocystis carinii. It may be given intravenously with prednisone for severe infection and those with low blood oxygen levels. Alternative drug treatments may include clindamycin phosphate (CleocinT), primaquine phosphate, and pentamidine isethionate (Pentan).
Residuals
Side effects of antibiotics are particularly common in people with AIDS. The death rate may range from 10 to 30 percent following treatment. Individuals with AIDS treated successfully for pneumocystis carinii require chronic use of medications to prevent recurrence.
Special Considerations
None.