6522 - Allergic or vasomotor rhinitis
DBQ: Link to Index of DBQ/Exams by Disability for DC 6522
Acronym: AR
Definition
Allergic rhinitis is an inflammatory disease involving the nasal mucous membranes. Other forms of rhinitis include:
{kind=link}
-
Vasomotor rhinitis which is chronic rhinitis characterized by intermittent vascular engorgement of the nasal mucous membrane, sneezing, and rhinorrhea. It is a mild, annoying chronic condition with continuous nasal obstruction, or continuous rhinorrhea.
-
Hayfever (pollinosis) which is an acute seasonal form of allergic rhinitis.
-
Perennial rhinitis, which is non-seasonal, may or may not be allergic, and symptoms vary throughout the year.
Etiology
Allergic rhinitis often occurs seasonally, when the pollen comes in direct contact with the respiratory mucosa. It may also occur perennially. Specific interactions between the IgE occur on the surface of the submucosal mast cells, which leads to the release of mediators and the subsequent symptoms. Complications from inflammatory or infectious sinusitis may result in maxillofrontal headaches, postnasal discharge, and persistent nasal stuffiness. Wind-borne pollens from trees, grass, and weeds usually induce hayfever, or primarily airborne fungal spores may cause it. Geographical differences may occur. The cause of vasomotor rhinitis is uncertain. It is characterized by periods of remission and exacerbation.
Signs & Symptoms
Mild symptoms of allergic rhinitis include: nasal pruritus, rhinorrhea, and sneezing. More severe symptoms include: violent, sudden, periodic attacks or recurring sneezing, and total obstruction of airflow caused by (copious) large amounts of mucus. Other symptoms include: tears, soreness of the eyes, irritability, fatigue, sluggishness and anorexia. Irritants such as cigarette smoke, aerosols, strong odors, perfumes, and insecticides may intensify the symptoms. The person may have inflammation of the lining of the eyelids, conjunctivitis, and pharyngitis.
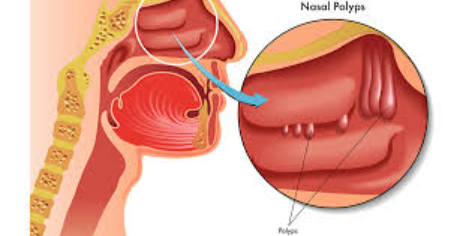
The physical findings of allergic rhinitis include: purplish-red mucous membranes; edematous turbinates, coated with thin, clear secretions; dark circles under the eyes; and mouth breathing caused by nasal congestion. Nasal polyps are usually uncommon in uncomplicated rhinitis. Periorbital edema, and fluid or retraction of the tympanic membrane may also be observed. Swollen tonsils, adenoids and cervical lymph nodes are uncommon in rhinitis, and this should indicate a need to search for complicating infections or other disease. Vasomotor rhinitis has no demonstrable allergies, polyps, infections, eosinophilia, or drug sensitivity. A dry atmosphere aggravates the condition. Symptoms of perennial rhinitis vary in severity through the year, with chronic nasal obstruction prominent, and which may extend to the eustachian tube.
{kind=link}
{kind=link}
Tests
A thorough history, including family history, and identification of IgE against the responsible allergen is done. Seasonal patterns of symptoms are noted and compared with local pollination. Specific IgE against various allergens is usually documented by skin testing or radioallergosorbent test (RAST). Normal or increased numbers of eosinophils in the peripheral blood and secretions are found. X-rays of the paranasal sinuses may be done. Vasomotor rhinitis is differentiated from specific viral and bacterial infections of the nose by the lack of purulent exudate and crusting. It is also differentiated from allergic rhinitis by the absence of identifiable allergens that cause the episodes. Conditions such as structural nasal abnormalities, endocrine abnormalities, or perennial non-allergic rhinitis of unknown causes must be ruled out by tests.
Treatment
Goals of treatment are to avoid offending allergens, or to reduce exposure to them, use of antihistamines or a combination of antihistamines and decongestants, and allergen immunotherapy. Care must be taken when prescribing sympathomimetic drugs in persons with cardiovascular disease because these agents can cause blood pressure and cardiac rates to increase. Topical corticosteroids may be used. Clinical improvement is noted after several days of treatment; however, maximum benefits may not be achieved for as long as two weeks. If the person is not responding satisfactorily to avoidance of offending allergens, or drug treatment, allergen immunotherapy may be used. Maximum efficacy with immunotherapy may take from two to three years. Treatment for vasomotor rhinitis may include humidified air, and systematic sympathomimetic amines, which are not recommended for long-term use. Topical vasoconstrictors are avoided.
Residuals
The person may have constant or recurring signs and symptoms. Treatment is long-term in avoiding allergens, and drug therapy is used for recurring episodes of symptoms. Immunotherapy may last from two to three years, or longer.
Special Considerations
-
Consider entitlement to service connection based on presumed exposure to fine particulate matter under 38 CFR 3.320
Notes
-
None.