8714 - The musculospiral nerve (radial nerve)-Neuralgia
DBQ: Link to Index of DBQ/Exams by Disability for DC 8714
Definition
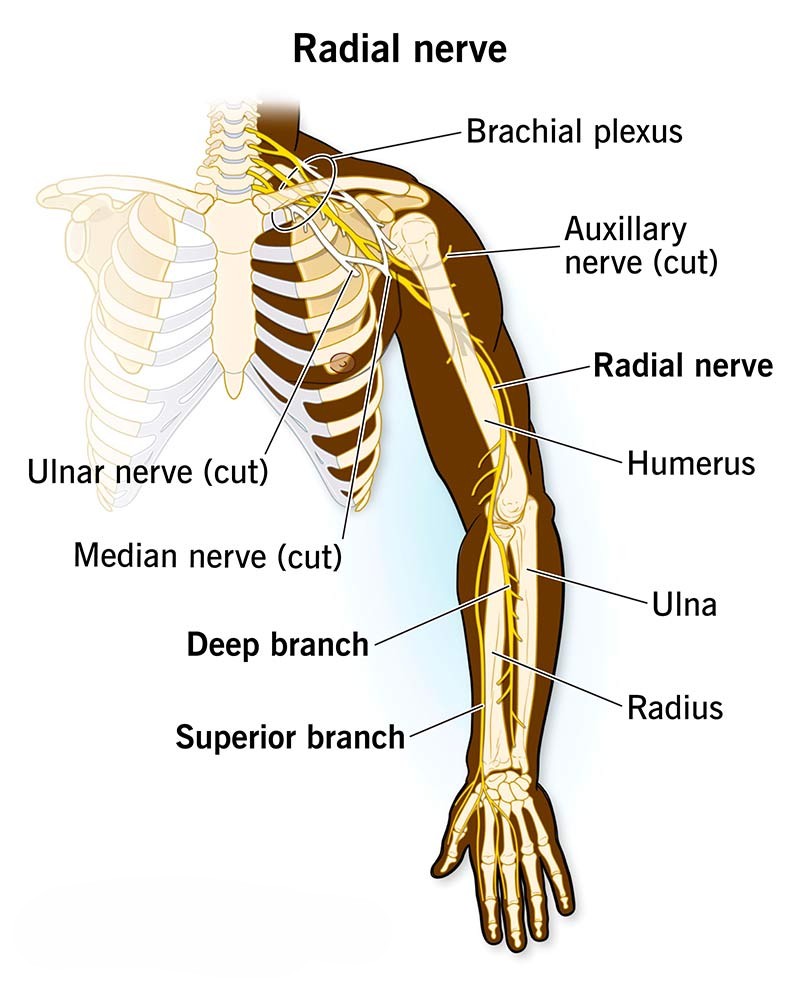
Neuralgia refers to a severe sharp pain occurring along the course of a nerve. The radial nerve, predominantly a motor nerve, arises from the middle trunk of the brachial plexus (see Diagnostic Code: 8711 Middle radicular group-Neuralgia). This nerve innervates the main extensors of the forearm, wrist, and fingers.
{kind=link}
Etiology
The middle third of the arm is the most common site of radial nerve injury. Although the cause of neuralgia may be unknown, attributing factors may be from injury or irritation to the nerve. These factors may include: lacerations; compression of the nerve from crutches, watchbands or handcuffs, prolonged elbow; extension; degenerative bone changes; tumors; and ganglia; or trauma such as a penetrating missile injury. Other causes may include: overextension of a joint; brachial neuritis; viral infections; and chronic degenerative diseases such as multiple sclerosis. Causes related to nerve damage may include: poor nutrition to the nerve, toxins, inflammation, infections, iatrogenic injection injuries, metabolic injury, nerve entrapment, or fractures.
Signs & Symptoms
Signs and symptoms may occur at irregular intervals. These manifestations may be characterized by attacks of unilateral, sharp, stabbing, or constant burning pain. Other symptoms may include: metabolic neuropathies, demyelination, triceps paralysis; loss of triceps reflex; weakness of forearm flexion; impaired elbow extension; elbow pain; a false weakness of finger flexion; weakness or paralysis of extension of the wrist, thumb and fingers; weakness of hand adduction; wrist drop; loss of grip; and loss of supination in forearm extension. Atrophy may develop with complete lesions of the nerve. There may be slight sensory loss localized to small areas of the hand, thumb, index, and middle fingers. There may be other signs and symptoms depending on involvement of neighboring nerves.
{kind=link}
Tests
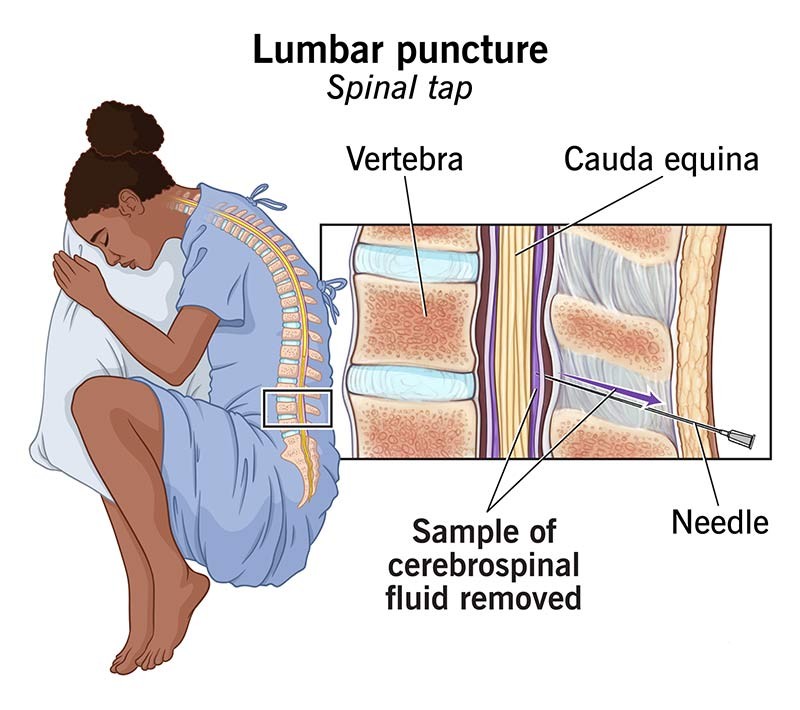
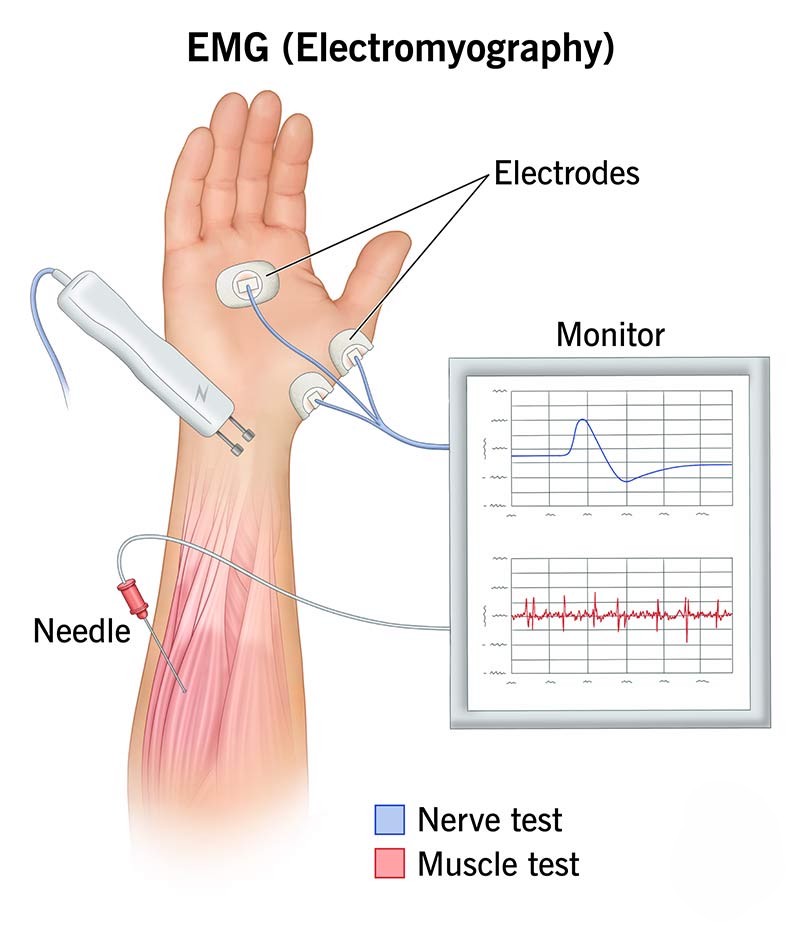
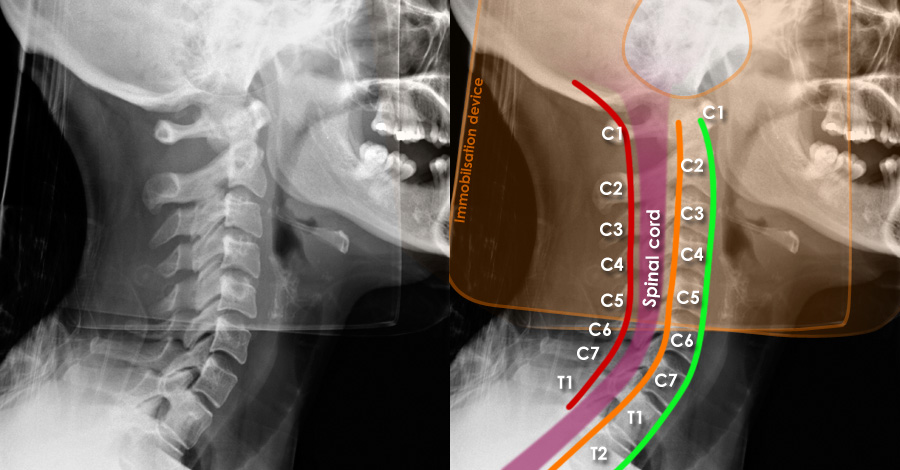
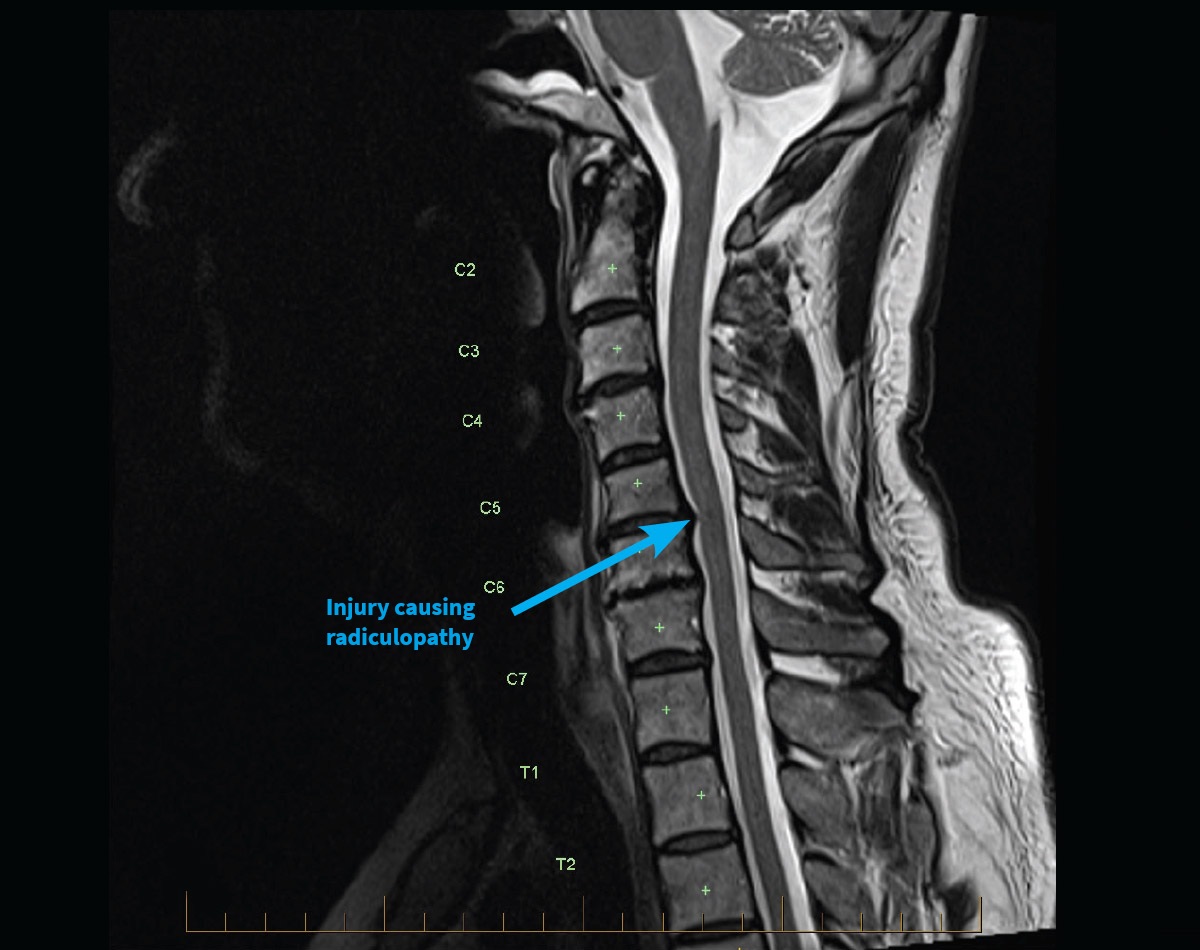
Diagnostic measures may include: a complete history; physical and neurological examinations; motor, sensory and reflex tests; blood studies; spinal tap; evoked responses; electromyography (EMG); x-ray; computed tomography (CT) scan; and magnetic resonance imaging (MRI).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment
Treatment may depend on the underlying cause. Measures for treatment may include: wrist splints; anti-inflammatory or pain medications; peripheral nerve blocks if pain medication fails; and transcutaneous electrical nerve stimulation (TENS). Physical therapy may be useful for certain types of neuralgia. Surgical resection may be necessary when medical therapy fails.
{kind=link}
Residuals
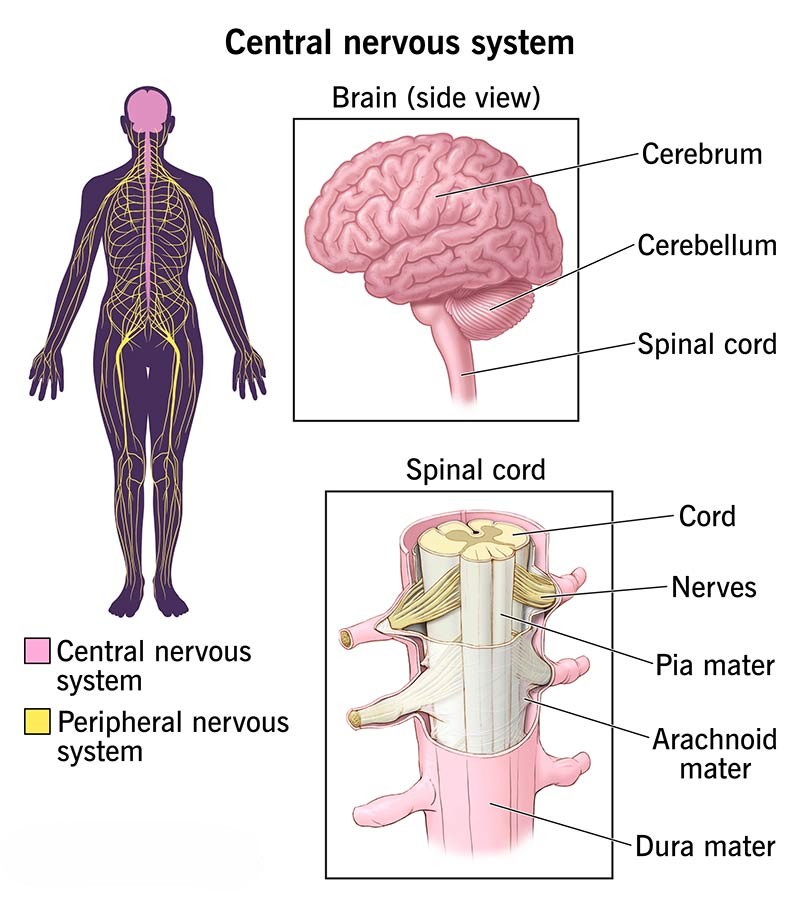
Regeneration of the nerve may depend on the degree and site of injury. The closer the injury is to the central nervous system (CNS), regeneration of a severely injured nerve is less likely to occur. Frequency of attacks may vary with periods of long remissions. However, remission periods may decrease with age. Continuous bouts may be incapacitating and may alter activities of daily living (ADL) and employment. As a result counseling intervention may be required. Painful paresthesias, dysesthesias, or neuromas of the wrist may develop. There may be a need for long-term pain management. Medications may warrant ongoing liver and blood studies. The potential for paralysis of the nerve exists.
{kind=link}
Special Considerations
-
If the Veteran is a former prisoner of war and was interned or detained for not less than 30 days, this disease shall be service connected if manifest to a degree of disability of 10% or more at any time after discharge or release from active military, naval, or air service even though there is no record of such disease during service, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied [38 CFR 3.309(c) Disease subject to presumptive service connection].
-
If the Veteran was exposed to an herbicide agent during active military, naval, or air service, this disease shall be service-connected if the requirements of 38 CFR 3.307(a)(6) are met even though there is no record of such disease during service, provided further that the rebuttable presumption provisions of 38 CFR 3.309(e). Disease subject to presumptive service connection.
Notes
-
Lesions involving only "dissociation of extensor communis digitorum," and "paralysis below the extensor communis digitorum," will not exceed the moderate rating under code 8514.