8526 - Anterior crural femoral-Paralysis of
DBQ: Link to Index of DBQ/Exams by Disability for DC 8526
Definition
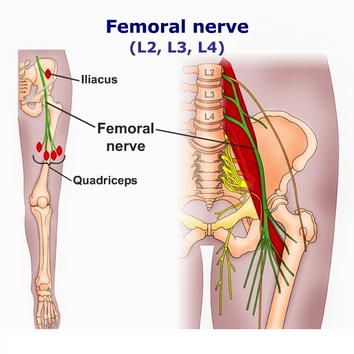
Paralysis refers to a temporary or permanent loss or impairment of motor or sensory function in a part. This code refers to the femoral nerve which arises from the 2nd, 3rd, and 4th lumbar nerves. Muscles of the lower torso and upper leg are innervated by this nerve. Cutaneous sensations are felt from the anterior surface of the thigh to the entire inner surface of the leg and the anterior internal surface of the knee.
{kind=link}
Etiology
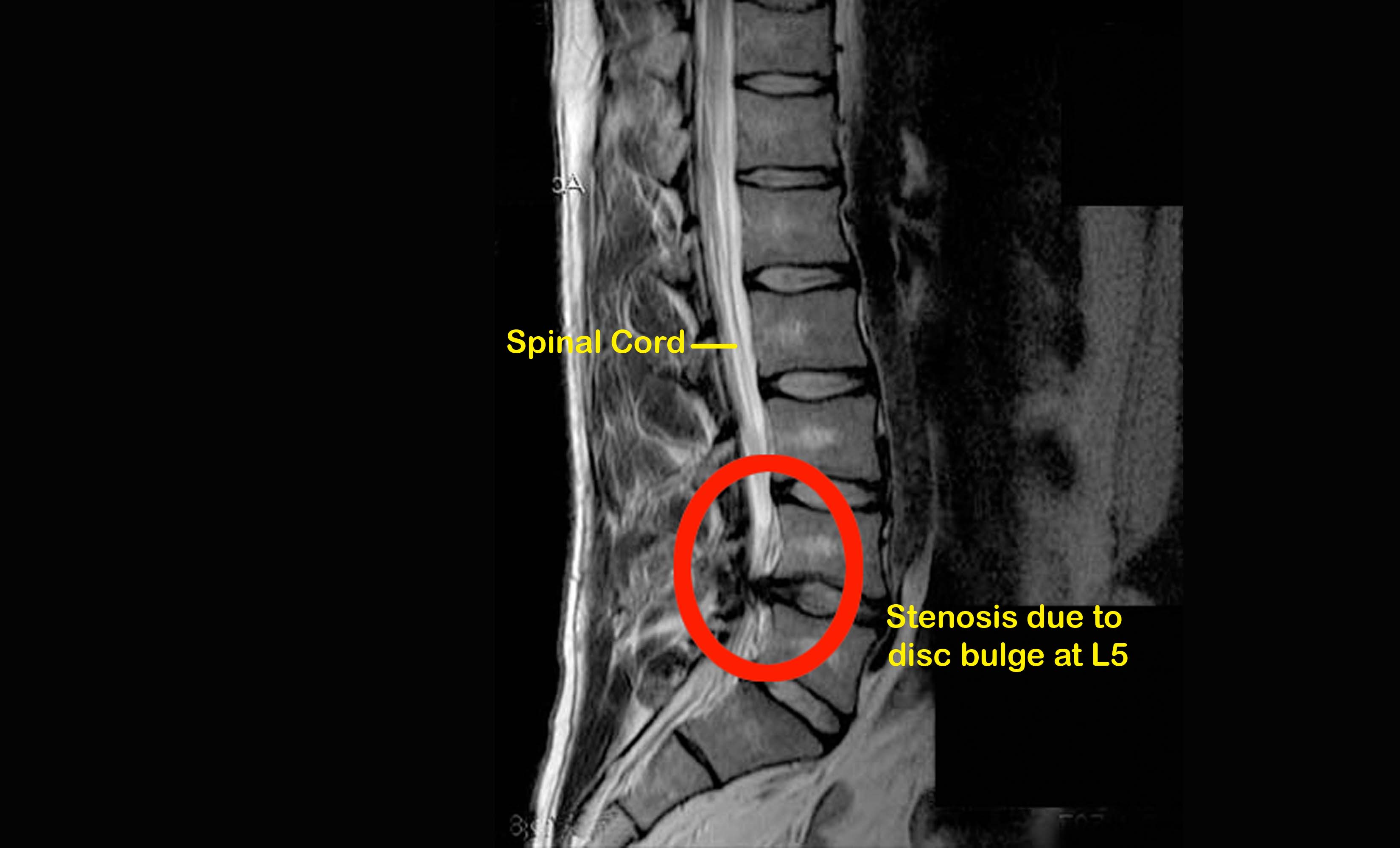
Paralysis may be caused by compression from tumors, or fractures of the pubic ramus or femur. Occasionally, an isolated incidence of femoral nerve palsy may be associated with gout, diabetes mellitus, or typhoid.
Signs & Symptoms
{kind=link}
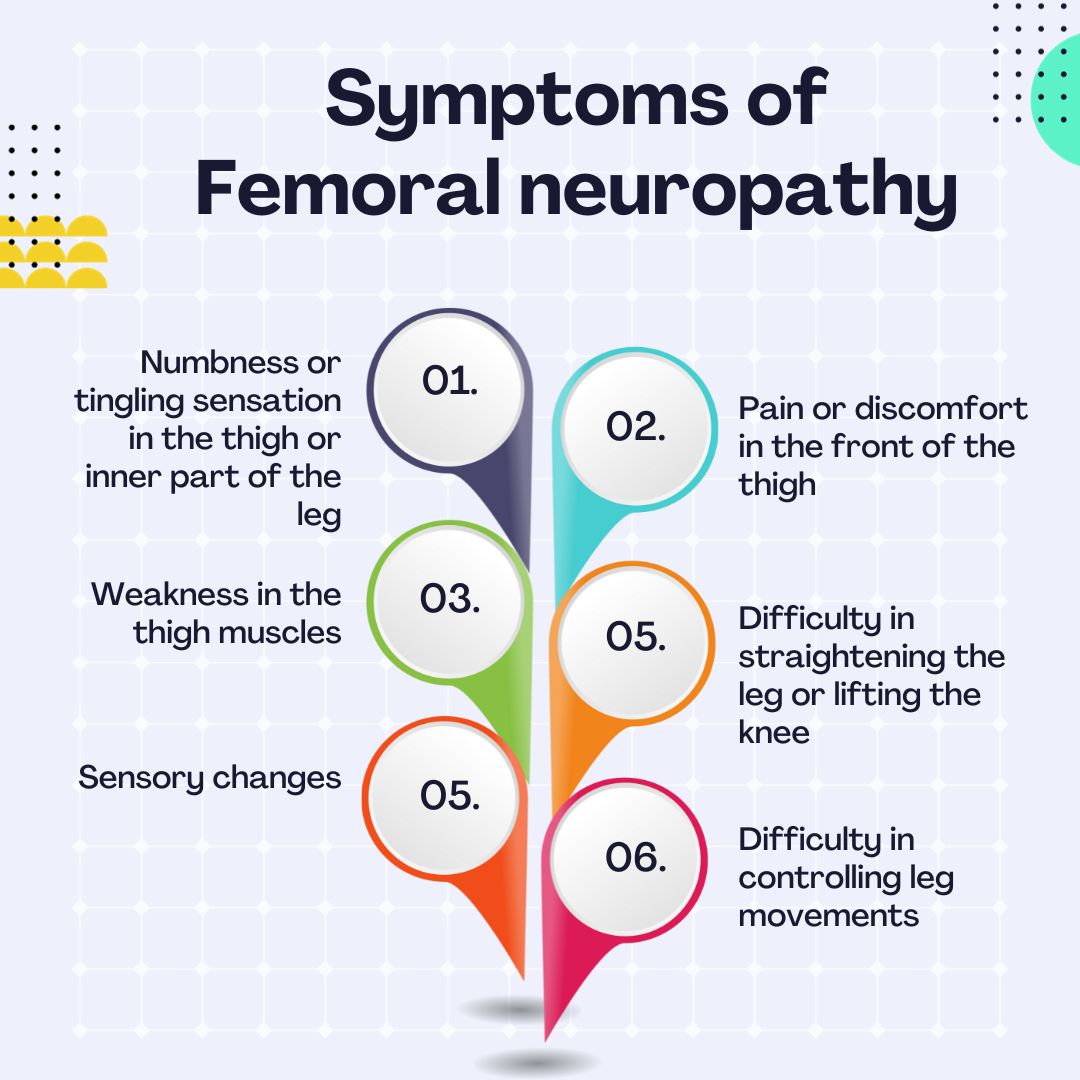
Injury to the nerve produces paralysis of leg extension, and weakness of hip flexion. Walking uphill or climbing stairs is almost impossible. Walking on flat ground is possible as long as the leg is extended; if there is any flexion the patient sinks down on a leg that suddenly bends. The quadriceps reflex is absent, and the skin sensation is impaired in an area smaller than the nerve distribution. Pain may be present in the thigh and rarely in the knee.
Tests
Paralysis must be distinguished from muscle atrophy that follow femur fractures or knee joint lesions. Peripheral nerve examination may include: nerve conduction tests; electromyography (EMG); computed tomography (CT) scan; magnetic resonance imaging (MRI); muscle-strength testing; deep tendon reflexes (DTR); sensory testing; and gait examination.
{kind=link}
{kind=link}
{kind=link}
Treatment
An orthopedic appliance that fixes the knee joint in extension is a valued treatment. If paralysis persists, then transplantation of the tendons may be considered. Other treatment measures may include the use of braces, crutches, a walker, physical therapy, analgesics, and electrical stimulation.
Residuals
Femoral nerve paralysis outcomes will depend upon whether the condition is temporary or permanent.
Special Considerations
-
If the Veteran is a former prisoner of war and was interned or detained for not less than 30 days, this disease shall be service connected if manifest to a degree of disability of 10% or more at any time after discharge or release from active military, naval, or air service even though there is no record of such disease during service, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied [38 CFR 3.309(c) Disease subject to presumptive service connection].
-
If the Veteran was exposed to an herbicide agent during active military, naval, or air service, this disease shall be service-connected if the requirements of 38 CFR 3.307(a)(6) are met even though there is no record of such disease during service, provided further that the rebuttable presumption provisions of 38 CFR 3.309(e). Disease subject to presumptive service connection.
-
Consider potential entitlement to special monthly compensation for loss of use of hand or foot when assigning the higher evaluations under particular Diagnostic Codes (e.g., Diagnostic Code 8510 through 8515, 8520, and 8521).
- This disability shall be granted service connection although not otherwise established as incurred in or aggravated by service if manifested to a compensable degree within the applicable time limits under 38 CFR 3.307 following service in a period of war or following peacetime service on or after January 1, 1947, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied. 38 CFR 3.309(a)
Notes
-
Neuritis, cranial or peripheral, characterized by loss of reflexes, muscle atrophy, sensory disturbances, and constant pain, at times excruciating, is to be rated on the scale provided for injury of the nerve involved, with a maximum equal to severe, incomplete, paralysis. See nerve involved for diagnostic code number and rating. The maximum rating which may be assigned for neuritis not characterized by organic changes referred to in this section will be that for moderate, or with sciatic nerve involvement, for moderately severe, incomplete paralysis. 38 CFR 4.123 Neuritis, cranial or peripheral.
-
With the exceptions noted, disability from the following diseases and their residuals may be rated from 10 percent to 100 percent in proportion to the impairment of motor, sensory, or mental function. Consider especially psychotic manifestations, complete or partial loss of use of one or more extremities, speech disturbances, impairment of vision, disturbances of gait, tremors, visceral manifestations, etc., referring to the appropriate bodily system of the schedule. With partial loss of use of one or more extremities from neurological lesions, rate by comparison with the mild, moderate, severe, or complete paralysis of peripheral nerves] 38 CFR 4.124a Schedule of ratings—neurological conditions and convulsive disorders.