8513 - All radicular groups-Paralysis of
DBQ: Link to Index of DBQ/Exams by Disability for DC 8513
Definition
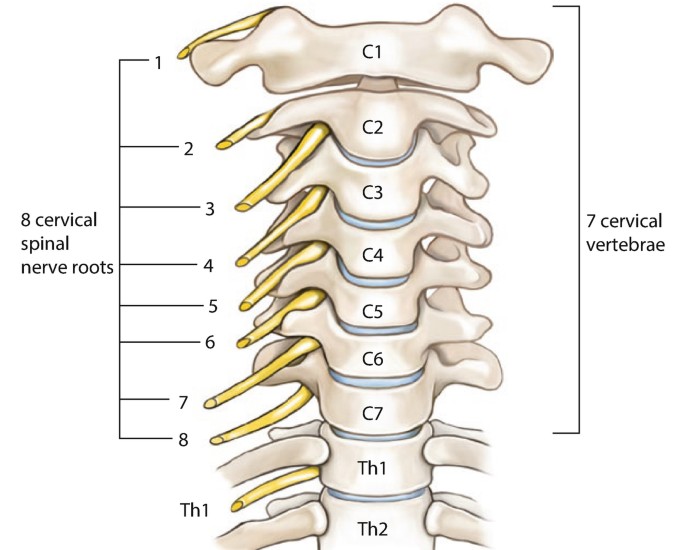
Paralysis refers to a temporary or permanent loss or impairment of motor or sensory function in a part. All radicular groups refer to the brachial plexus. The brachial plexus is formed by the 5th, 6th, 7th and 8th cervical roots, and first thoracic root which form an upper, middle, and lower trunk. (See Diagnostic Code: 8510 Upper radicular group-Paralysis of, Diagnostic Code: 8511 Middle radicular group-Paralysis of, and Diagnostic Code: 8512 Lower radicular group-Paralysis of.)
{kind=link}
Etiology
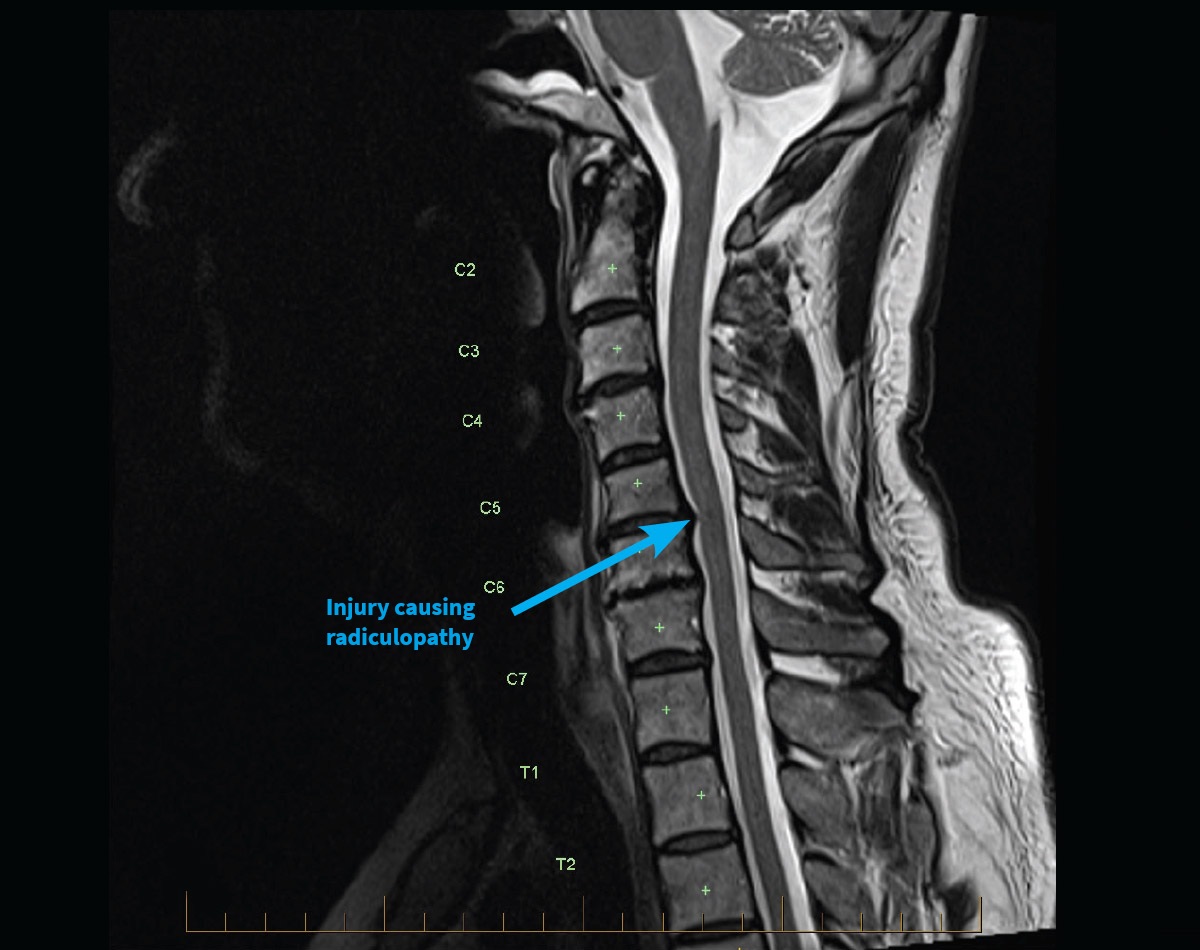
Paralysis of these nerves may be caused by damage to the nerve fibers, cell body, or myelin sheath. Causes of damage may include: trauma; penetrating missile injury; shoulder injury; traction injuries; overextension of a joint; brachial neuritis; carrying heavy objects supported at the shoulder; iatrogenic injection injuries; metabolic injury; infection; and compression of the nerve from degenerative bone changes, nerve entrapment, fractures, irradiation, or tumors.
Signs & Symptoms
Signs and symptoms may depend on the affected root or roots and involvement of neighboring nerves. Manifestations may include: inability to raise the arm at the shoulder; triceps weakness; decreased or loss of reflexes; pain; moderate to severe muscle weakness; and muscle atrophy. In addition, there may be elbow pain; inability to extend the elbow, wrist, fingers and thumb; weakness of adduction of the hand; and wrist drop. Other evidence may include: paralysis of forearm and finger flexion, and of abduction and internal rotation and external rotation of the arm. There may be distal paresthesias and pain with partial sensory loss to confined areas of the outer arm, forearm, hand, thumb or index and middle fingers, and an inability to use a normal functioning hand. There may be vascular symptoms such as swelling, blanched fingers, an aching, cold and cyanotic arm. Raynaud's disease may be rarely present.
{kind=link}
Tests
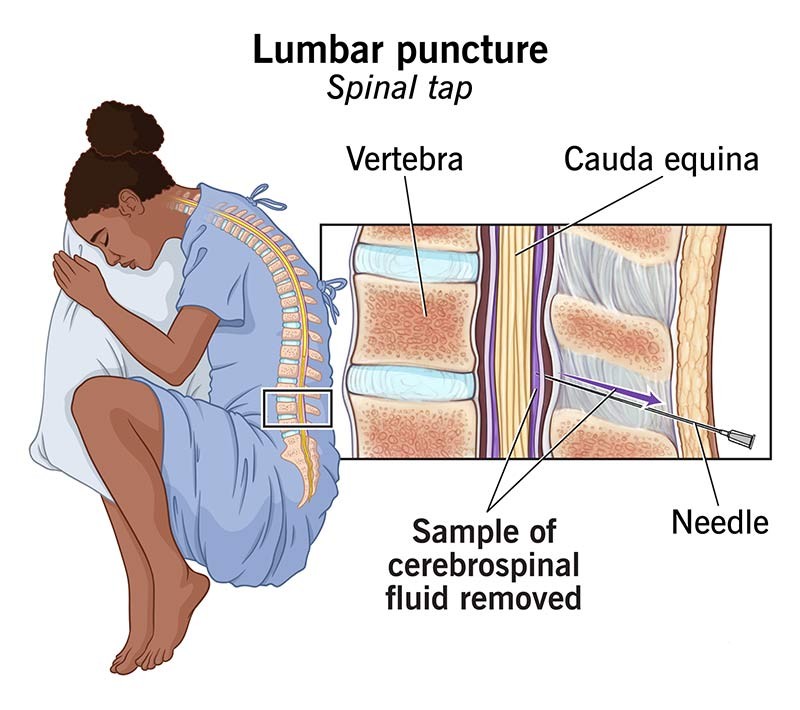
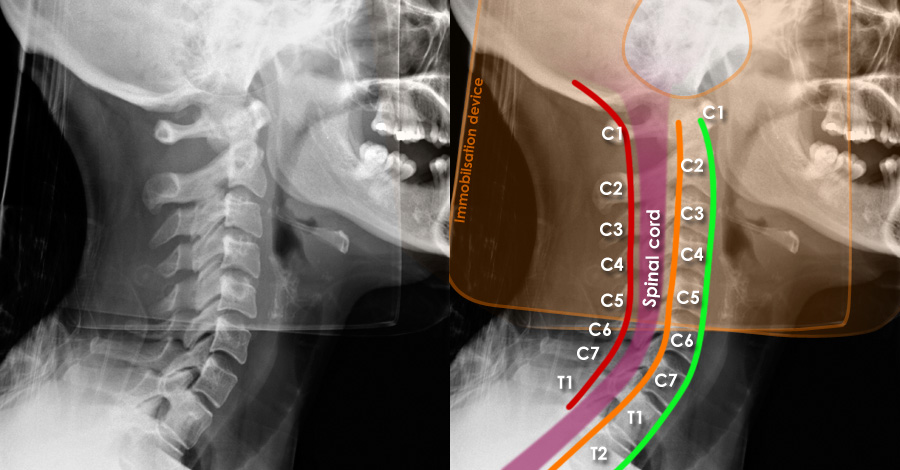
Diagnostic measures may include: a complete history; physical and neurological examinations; motor, sensory, and reflex tests; strength and resistance tests; blood studies; spinal tap; evoked responses; electromyography (EMG); x-ray; computed tomography (CT) scan; and magnetic resonance imaging (MRI).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment
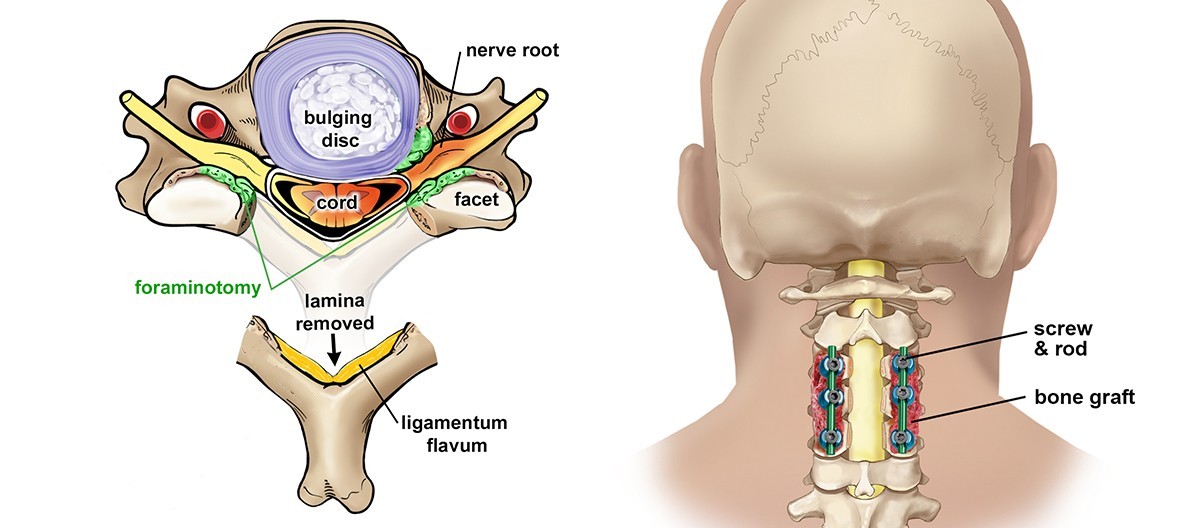
Treatments may include management of the underlying disorder. Other measures of treatment may include: splints; physical therapy; anti-inflammatory or pain medications; transcutaneous electrical nerve stimulation (TENS); or, in some cases, surgery may be needed.
{kind=link}
{kind=link}
Residuals
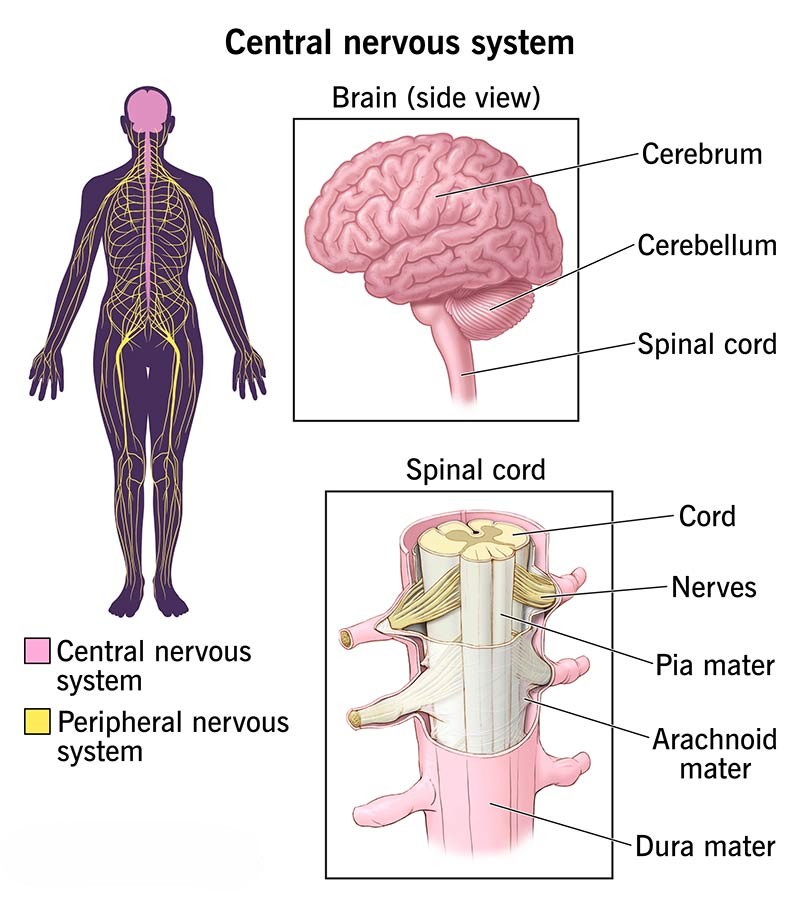
Regeneration may depend on the degree of axonal injury and site of injury. The closer the injury is to the central nervous system (CNS), regeneration of a severely damaged nerve is less likely to occur. Recovery may range from return to complete function to permanent dysfunction. Recovery from weakness may take several months. In compression injury, complete recovery may take weeks depending on the length and severity of compression. There may be severe limitations in shoulder and elbow joint mobility from lack of use, and a potential for contractures to develop. Supination may be possible via the action of the biceps. In the presence of triceps paralysis, forearm extension may be achieved via gravity. There may be injuries to other distal peripheral nerves. Pain may be provoked when carrying heavy items in the hand. Intensive rehabilitation may be delayed for certain injuries. Long-term physical therapy may be needed. There may be alteration of employment and daily activities requiring counseling intervention.
{kind=link}
Special Considerations
-
If the Veteran is a former prisoner of war and was interned or detained for not less than 30 days, this disease shall be service connected if manifest to a degree of disability of 10% or more at any time after discharge or release from active military, naval, or air service even though there is no record of such disease during service, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied [38 CFR §3.309(c) Disease subject to presumptive service connection].
-
If the Veteran was exposed to an herbicide agent during active military, naval, or air service, this disease shall be service-connected if the requirements of 38 CFR 3.307(a)(6) are met even though there is no record of such disease during service, provided further that the rebuttable presumption provisions of 38 CFR 3.309(e). Disease subject to presumptive service connection.
-
Consider potential entitlement to special monthly compensation for loss of use of hand or foot when assigning the higher evaluations under particular Diagnostic Codes (e.g., Diagnostic Code 8510 through 8515, 8520, and 8521).
Notes
-
POW presumptive provisions apply to peripheral neuropathy except where directly related to infectious causes.