8405 - Fifth (trigeminal) cranial nerve-Neuralgia
DBQ: Link to Index of DBQ/Exams by Disability for DC 8405
Definition
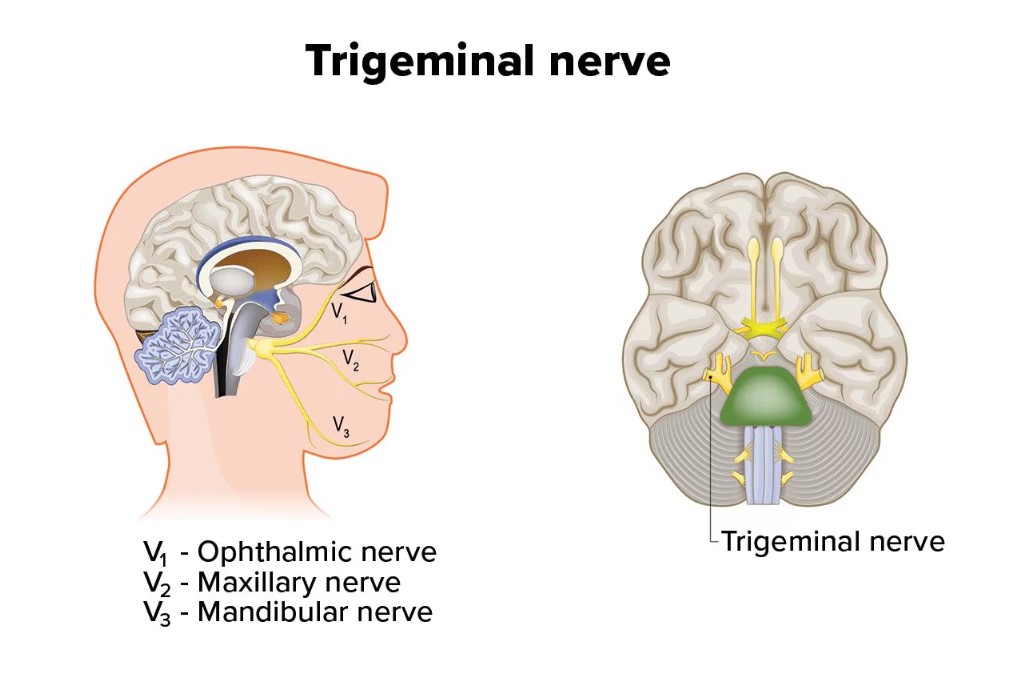
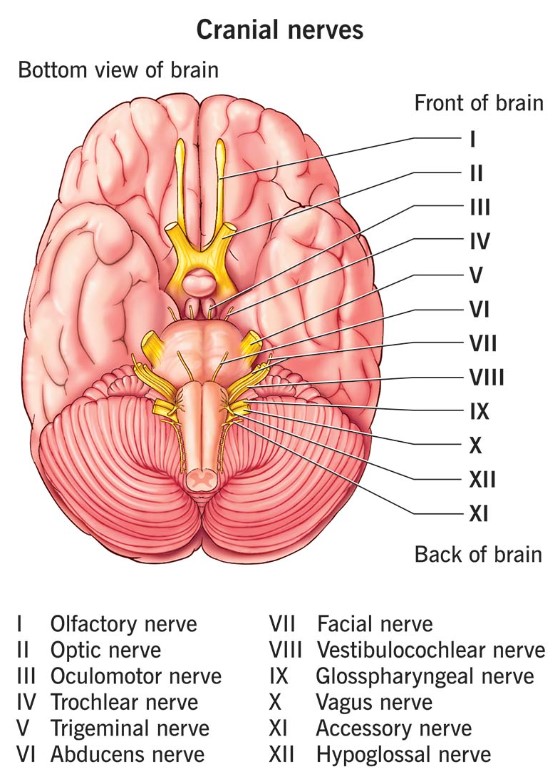
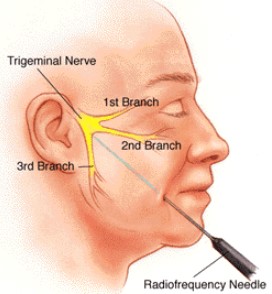
Neuralgia refers to severe sharp pain occurring along the course of a nerve. The Vth cranial nerve is one of twelve pairs of nerves connected with the brain, which supplies sensation to the skin of the face and front half of the head, as well as innervating the masseter and pterygoid masticatory muscles. The nerve also provides sensory input from the eye surface, tear glands, and upper eyelids. In this case, trigeminal neuralgia refers to the disorder, tic douloureux.
{kind=link}
{kind=link}
Etiology
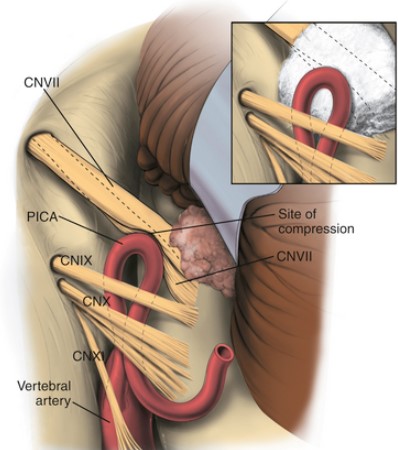
Although the most frequent of all neuralgias, the cause of neuralgia of the Vth cranial nerve may be unknown. Attributing causes may include: injury or irritation to the nerve; nerve root compression by a blood vessel or tumor; viral infections; lesions in the brain stemming from multiple sclerosis; or vascular lesions involving the Vth nerve root. In addition, reported fibrotic changes in the gasserian ganglion may be a possible contributing cause.
Signs & Symptoms
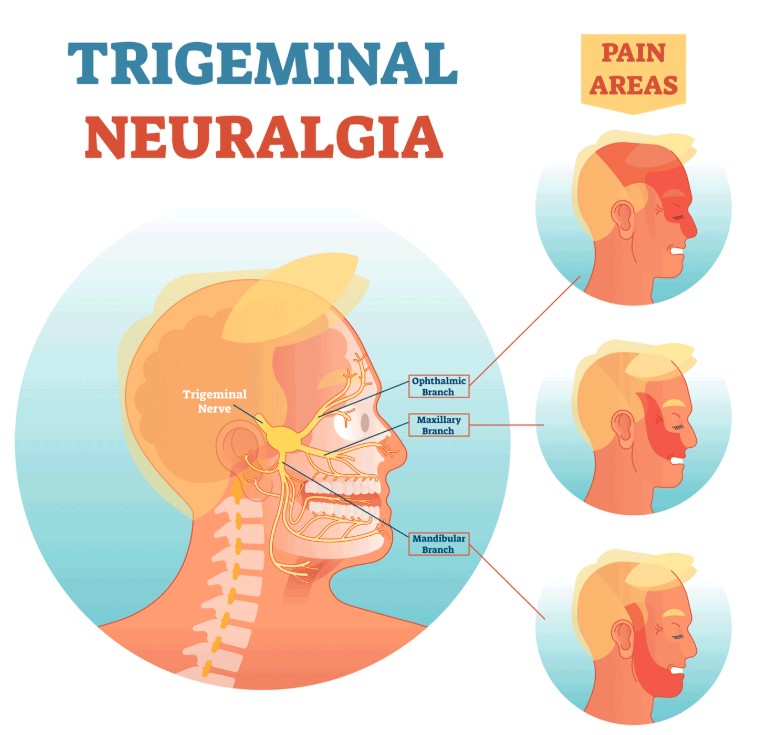
Symptoms may be characterized by recurrent paroxysms of excruciating, sharp, searing, lightning-like jabs and stabbing pain, or constant burning pain in the lips, gums, cheek, chin or forehead, occurring in one or more branches of the nerve distribution. Additional manifestations may include: hyperesthesia of the face without loss of cutaneous sensation; and rubbing or pinching of the face by the patient. There may be presence of a trigger zone with hypersensitivity to light touch of the cheeks, gums or tip of the nose. Facial movement or chewing may also provoke the trigger zone. As a result, there may be decreased nutritional intake and lack of facial expressions. Additionally, trigeminal neuralgia may be characterized by remission from short duration to absence of attacks lasting months to years. The remissions may become shorter with aging. Attacks may be bilateral, but usually occur on one side (the right side more than the left) of the face, and are brief (15 to 60 seconds). Frequency of attacks may vary from many per day to a few times per month.
{kind=link}
Tests
Physical and neurological examinations are indicated. Diagnosis may usually be made from the history and physical examination, and the patient's description and demonstration of the site of origin and spread of pain. X-rays, magnetic resonance imaging (MRI) or computed tomography (CT) scan may be used to rule out other diagnoses. In addition, evoked potential testing and cerebrospinal fluid (CSF) testing may be done.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment
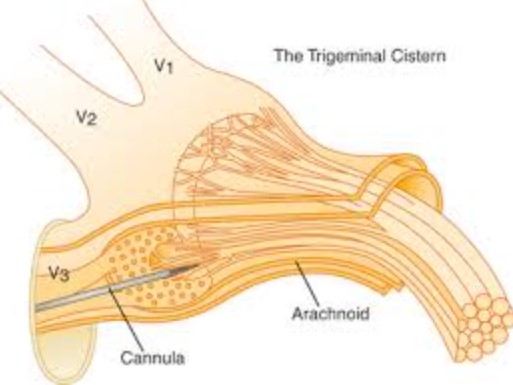
Medication for pain management may be given. Peripheral nerve blocks may be done if pain medication fails. Oral or intravenous injection of anticonvulsants may interrupt episodes. Muscle relaxants, such as baclofen, may also be used alone or in conjunction with anticonvulsants. In some cases, surgery may be indicated, but may not be a satisfactory course of treatment. Preferred treatments may include: extracranial percutaneous thermal destruction of the affected nerve branch; percutaneous radio frequency trigeminal gangliolysis (PRTG); percutaneous retrogasserian glycerol rhizotomy (PRGR); as well as decompression of anomalous vessels from the nerve root.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Residuals
Continuous bouts of neuralgia may be incapacitating. Medications may warrant ongoing liver and blood studies. There may be social isolation from fear of attacks. Nutritional status may decline, and nutritional counseling, as well as emotional support may be needed.
Special Considerations
-
This disease shall be granted service connection although not otherwise established as incurred in or aggravated by service if manifested to a compensable degree within the applicable time limits under 38 CFR 3.307 following service in a period of war or following peacetime service on or after January 1, 1947, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied [38 CFR 3.309 [Disease subject to presumptive service connection], 38 CFR 3.309(a). [chronic disease].
Notes
-
Tic douloureux may be rated in accordance with seventy, up to complete paralysis.
-
Dependent upon relative degree of sensory manifestation or motor loss.
-
Disability from lesions of peripheral portions of first, second, third, fourth, sixth, and eighth nerves will be rated under the Organs of Special Sense. The ratings for the cranial nerves are for unilateral involvement; when bilateral, combine but without the bilateral factor.
-
Neuralgia, cranial or peripheral, characterized usually by a dull and intermittent pain, of typical distribution so as to identify the nerve, is to be rated on the same scale, with a maximum equal to moderate incomplete paralysis. See nerve involved for diagnostic code number and rating. Tic douloureux, or trifacial neuralgia, may be rated up to complete paralysis of the affected nerve. (38 CFR 4.124)