8211 - Eleventh (spinal accessory, external branch) cranial nerve-Paralysis of
DBQ: Link to Index of DBQ/Exams by Disability for DC 8211
Definition
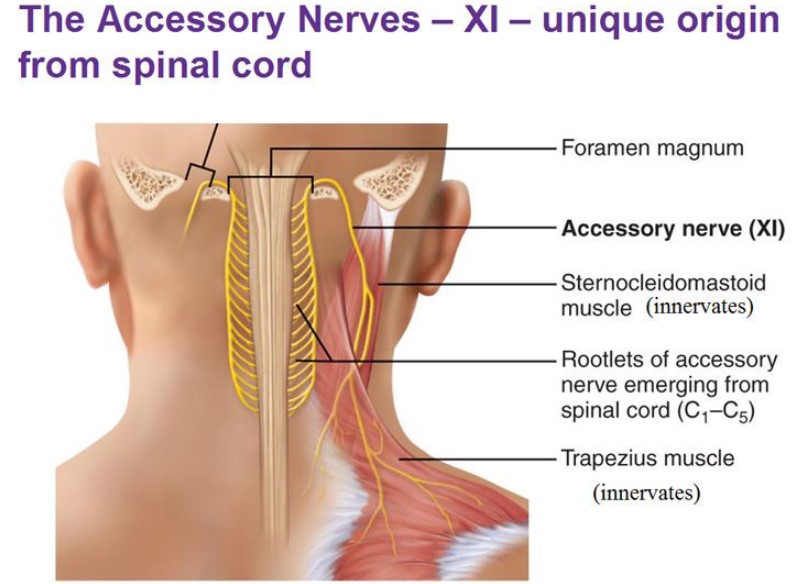
Paralysis refers to a temporary or permanent loss or impairment of motor or sensory function in a part. The XIth cranial nerve, also known as the accessory nerve, is one of twelve pairs of nerves connected with the brain. It supplies the trapezius and sternocleidomastoid muscles, and the pharynx. The cranial nerve is a motor nerve that acts to turn the head and shrug the shoulders.
{kind=link}
{kind=link}
Etiology
Paralysis of this nerve may be caused by tumors at the base of the skull, and the meninges. Other causative factors include: lesions of the nerve or nerve root; brainstem lesions or injury; aneurysms; surgery; and infections. Deficits of this nerve may be in combination with those of the IXth and Xth cranial nerves. (See Diagnostic Code: 8210 Tenth [pneumogastric, vagus cranial nerve-Paralysis of], and Diagnostic Code: 8209 Ninth [glossopharyngeal] cranial nerve-Paralysis of).
Signs & Symptoms
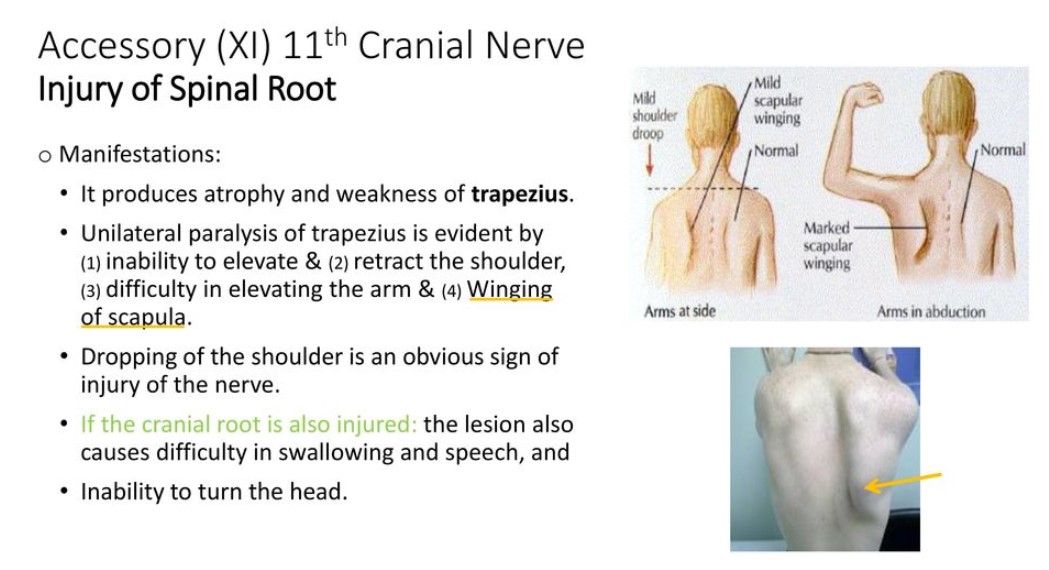
Manifestations may include: partial or complete paralysis of the sternocleidomastoid and trapezius muscles; drooping of the shoulders, or winging of the scapula that is displaced toward the affected side; muscle atrophy; weakness; and inability to rotate the head away from the affected side.
{kind=link}
Tests
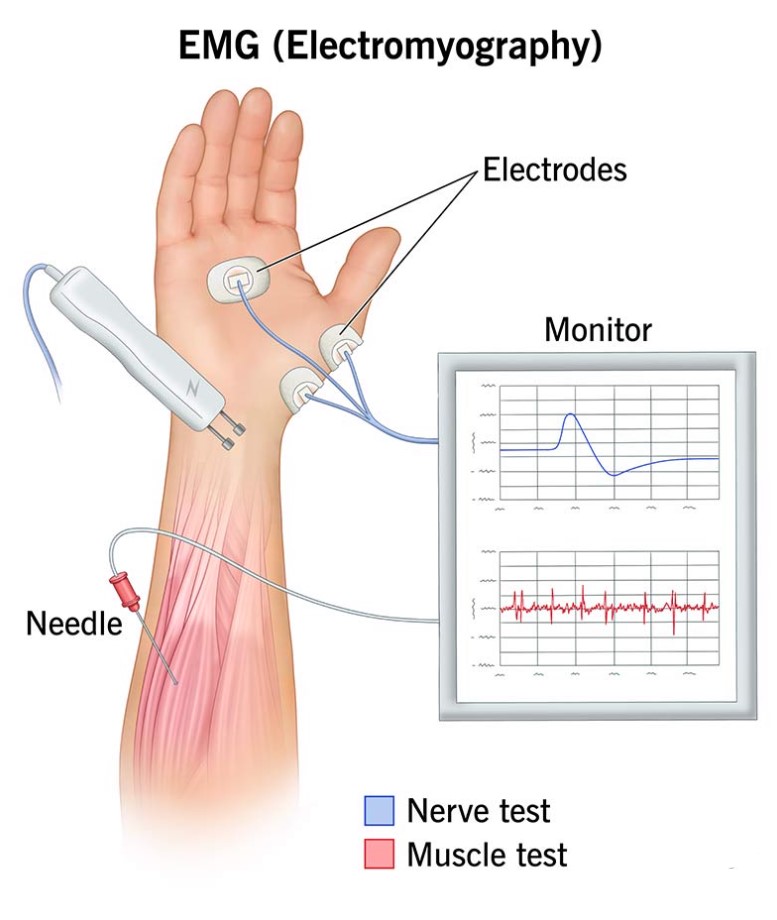
Diagnostic measures may include: a complete history; physical and neurological examinations; motor tests; blood studies; spinal tap; computed tomography (CT) scan; magnetic resonance imaging (MRI); and electromyography (EMG).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment
Treatment may be directed to the specific underlying cause and symptoms. Possible components of the treatment plan include: surgery; medications to treat underlying diseases or infection; and physical therapy. Other treatments for symptoms of affected neighboring nerves may be indicated.
{kind=link}
Residuals
Regeneration of the nerve may depend on the degree and site of injury. The closer the injury is to the central nervous system (CNS), regeneration of a severely damaged nerve is less likely to occur. Partial paralysis may be progressive and become permanent. Although most patients recover, accessory neuropathies may be recurrent. There may associated injury to neighboring nerves.
Special Considerations
-
This disease shall be granted service connection although not otherwise established as incurred in or aggravated by service if manifested to a compensable degree within the applicable time limits under 38 CFR 3.307 following service in a period of war or following peacetime service on or after January 1, 1947, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied [38 CFR 3.309 [Disease subject to presumptive service connection], 38 CFR 3.309(a). [chronic disease].
Notes
-
Dependent upon loss of motor function of sternomastoid and trapezius muscles.
-
Disability from lesions of peripheral portions of first, second, third, fourth, sixth, and eighth nerves will be rated under the Organs of Special Sense. The ratings for the cranial nerves are for unilateral involvement; when bilateral, combine but without the bilateral factor.