5235 - Vertebral fracture or dislocation
DBQ: Link to Index of DBQ/Exams by Disability for DC 5235
Acronym: FX (fracture)
Definition
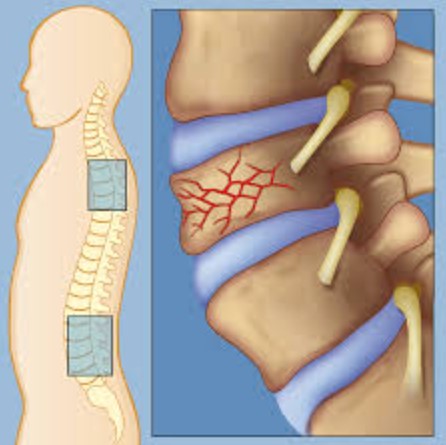
A break in a bone refers to a fracture. Dislocation is the displacement of any part, especially the temporary displacement of a bone from its normal position in a joint. In this case, the fracture or dislocation occurs at some point in a vertebra.
{kind=link}
Etiology
Generally, spinal injuries result from traumatic events, e.g., motor vehicle accidents, falls, sports-like diving into shallow water, acts of violence i.e. gunshot wounds, etc. A break in this area can be dangerous if there is damage to the spinal cord. In older patients (75 years or older) falls account for 60% of spinal fractures. Males are injured four times more frequently than females. Osteoporosis are the most common precipitating factor for vertebral fracture. However, trauma, cancer, chemotherapy, infection, long-term steroid use, hyperthyroidism, and radiation therapy are also known to weaken bones that can lead to compression fractures.
Signs & Symptoms
{kind=link}
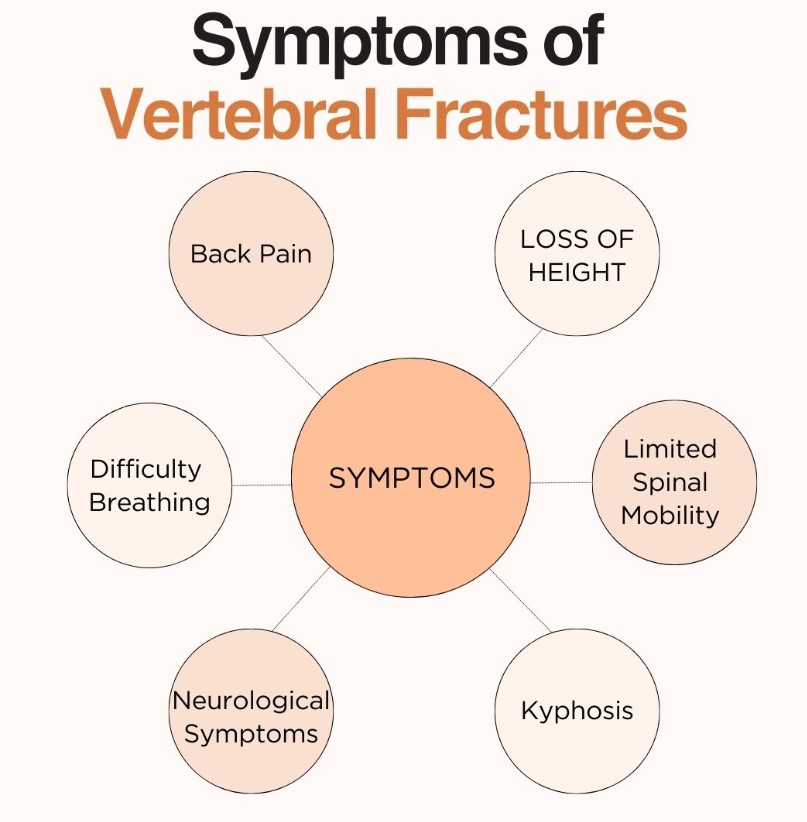
Veterans will most likely complain of muscle spasm and back pain that worsens with movement. If the cervical vertebra is involved, pain may result in point tenderness. Inability to move the neck or pain on motion requires careful immobilization of the head and neck until adequate exam and x-rays are completed. Weakness, numbness, or paralysis of the arms, hands, or feet warrants a presumptive diagnosis of spinal cord injury until proven otherwise. In lumbar fractures, pain may radiate to other areas, e.g., as to the legs.
Tests
Spinal x-rays detect the fracture, and computed tomography (CT) scan and magnetic resonance imaging (MRI) provide added information. Careful sensory/ motor exam should complement rectal exam, particularly if a spinal cord injury is suspected. Spinal shock (i.e. the absence of all spinal reflexes, below a spinal cord injury) usually ends in 24 hours, and will help determine a complete or partial injury.
{kind=link}
{kind=link}
{kind=link}
Treatment
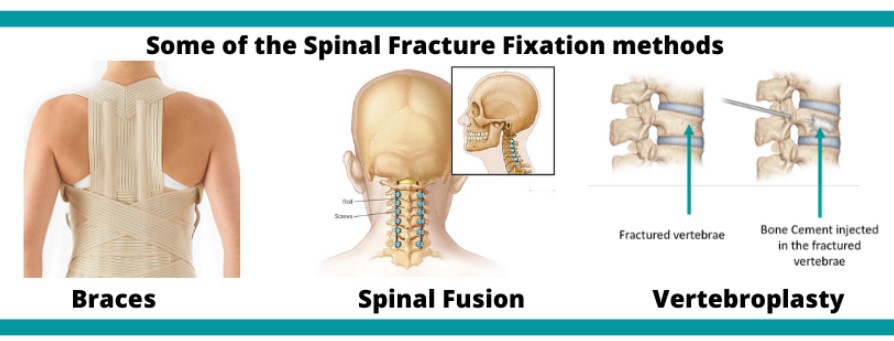
Initially, the patient is immobilized for stabilization and prevention of spinal cord damage. The treatments generally instituted include: casts; surgery; traction with tongs in the skull; halo devices; and medications for discomfort and muscle tension. High dose corticosteroids given within 8 hours of injury has been shown to improve neurologic function (motor and sensory) at 6 weeks and 6 months post injury, even in complete spinal cord injuries.
{kind=link}
Residuals
Initially, the patient is immobilized for stabilization and prevention of spinal cord damage. The treatments generally instituted include: casts; surgery; traction with tongs in the skull; halo devices; and medications for discomfort and muscle tension. High dose corticosteroids given within 8 hours of injury has been shown to improve neurologic function (motor and sensory) at 6 weeks and 6 months post injury, even in complete spinal cord injuries.
Special Considerations
-
The rating schedule for musculoskeletal was updated on February 7, 2021. Protection still does apply and should be considered with existing evaluations (38 CFR 3.951(a)).
-
Evaluate under the General Rating Formula for Diseases and Injuries of the Spine for diagnostic codes 5235 to 5243 unless 5243 is evaluated under the Formula for Rating Intervertebral Disc Syndrome Based on Incapacitating Episodes.
Notes
-
Evaluate any associated objective neurologic abnormalities, including, but not limited to, bowel or bladder impairment, separately, under an appropriate diagnostic code.
-
For VA compensation purposes, normal forward flexion of the cervical spine is zero to 45 degrees (see forward flexion-cervical spine), extension is zero to 45 degrees (see extension-cervical spine), left and right lateral flexion are zero to 45 degrees (see lateral flexion-cervical spine), and left and right lateral rotation are zero to 80 degrees (see lateral rotation-cervical spine). Normal forward flexion of the thoracolumbar spine is zero to 90 degrees , extension is zero to 30 degrees (see forward flexion-thoracolumbar spine), left and right lateral flexion are zero to 30 degrees (see lateral flexion-thoracolumbar), and left and right lateral rotation are zero to 30 degrees (see lateral rotation-thoracolumbar spine). The combined range of motion refers to the sum of the range of forward flexion, extension, left and right lateral flexion, and left and right rotation. The normal combined range of motion of the cervical spine is 340 degrees and of the thoracolumbar spine is 240 degrees. The normal ranges of motion for each component of spinal motion provided in this note are the maximum that can be used for calculation of the combined range of motion.
-
In exceptional cases, an examiner may state that because of age, body habitus, neurologic disease, or other factors not the result of disease or injury of the spine, the range of motion of the spine in a particular individual should be considered normal for that individual, even though it does not conform to the normal range of motion stated in Note (2). Provided that the examiner supplies an explanation, the examiner's assessment that the range of motion is normal for that individual will be accepted.
-
Round each range of motion measurement to the nearest five degrees.
-
For VA compensation purposes, unfavorable ankylosis is a condition in which the entire cervical spine, the entire thoracolumbar spine, or the entire spine is fixed in flexion or extension, and the ankylosis results in one or more of the following: difficulty walking because of a limited line of vision; restricted opening of the mouth and chewing; breathing limited to diaphragmatic respiration; gastrointestinal symptoms due to pressure of the costal margin on the abdomen; dyspnea or dysphagia; atlantoaxial or cervical subluxation or dislocation; or neurologic symptoms due to nerve root stretching. Fixation of a spinal segment in neutral position (zero degrees) always represents favorable ankylosis.
-
Separately evaluate disability of the thoracolumbar and cervical spine segments, except when there is unfavorable ankylosis of both segments, which will be rated as a single disability.