9416 - Dissociative amnesia; dissociative identity disorder
DBQ: Link to Index of DBQ/Exams by Disability for DC 9416
Definition
A disorder characterized by a person's behavior being alternately taken over by two or more personalities. The disorder also involves an inability to recall personal information relating to some of the personalities.
{kind=link}
Etiology
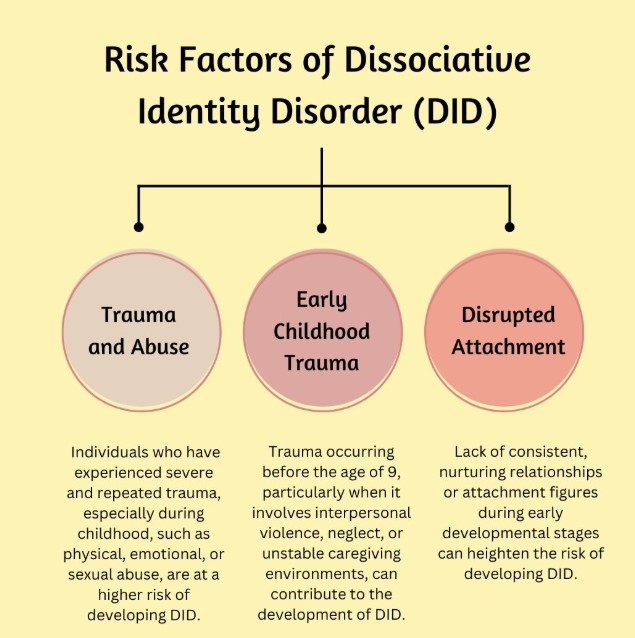
The disorder is believed to be caused by several factors: overwhelming stress, a capacity to dissociate, the use of defense processes, lack of nurturing during childhood, and lack of protection in overwhelming situations. Identity in children must be formed as a developmental task. If the child is overwhelmed, the task is obstructed and a unified identity does not occur. Ninety-eight percent of the adults with this disorder report abuse as a child. War and disaster may play a role in this developmental disorder. In addition, loss of a parent, or a child who requires many hospitalizations and operations may be overwhelming.
{kind=link}
Signs & Symptoms
{kind=link}
This disorder tends to mimic other psychiatric disorders. These patients often, have been treated several times for different diagnoses and treatment has failed. Most patients experience some symptoms of depression, anxiety, panic attacks, eating disorders, posttraumatic stress, sexual dysfunction and self-injury with suicide attempts. Two characteristic symptoms are:
-
Depersonalization - a feeling of being removed from oneself
-
Derealization - the experiencing of familiar persons and surroundings as strange and unfamiliar.
Tests
Diagnosis is usually made with medical and psychiatric evaluation. The psychiatrist may attempt to bring forth the other personality or personalities for which the person had amnesia. Drug-induced interviews or hypnosis may be used to explore the dissociative phenomena, and patients are asked to keep a personal log between visits. The diagnostic criteria are as follows:
{kind=link}
-
The presence of two or more distinct identities or personality states.
-
At least two of these identities or personality states recurrently take control of the person's behavior.
-
Inability to recall vital personal information and it is too extensive to be attributed to ordinary forgetfulness.
-
The disorder is not due to the effects of a substance or a general medical condition.
Treatment
The treatment goal is to achieve integration; however, this disorder does not go away spontaneously. Treatment includes two or more psychotherapy sessions a week for 3 to 6 years. The therapy is divided into three phases:
-
Initially, safety is a priority; the patient is stabilized and then strengthened to deal with the difficult issues and problem personalities.
-
In the second phase, the patient is assisted to deal with the painful issues and grieve over the losses. When the reason for the dissociation is addressed, the patient can move into the final phase.
-
The final phase is focused on reconnecting and integrating. The patient's selves and relationships are rehabilitated and social functioning is re-instituted. Hypnotic suggestion or imagery is used to help unify these personalities. When integration is attained, treatment will continue in order to deal with unresolved issues.
Residuals
Most patients continue to see their psychiatrist and do not terminate therapy because the service members have come to think of the psychiatrist as necessary to help deal with issues.
Special Considerations
-
If a Veteran is a former prisoner of war, this disease shall be service connected if manifest to a degree of disability of 10% or more at any time after discharge or release from active military, naval, or air service even though there is no record of such disease during service, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied [38 CFR 3.309(c) Disease subject to presumptive service connection].
-
May be entitled to special monthly compensation where the Veteran has a single service-connected disability rated as 100% with additional service-connected disability or disabilities independently ratable at 60% or more, which are separate and distinct from the 100% service-connected disability and involves different anatomical segments or bodily systems. See 38 CFR 3.350(i)(1) – Special Monthly Compensation (SMC).
-
Competency must be addressed in cases where a mental condition is initially evaluated as totally disabling or when the total evaluation is continued in a rating decision. This includes when individual unemployability is awarded or continued on the basis of a single mental health disability, and when assigning or continuing a temporary total evaluation for a mental disorder under 38 CFR 4.29 [38 CFR 3.353 [Determinations of incompetency and competency]].
-
Reference 38 CFR 3.384 for the applicability of the term psychosis.
-
Review 38 CFR 3.354 with regard to determinations of insanit
Notes
-
An incapacitating episode is a period during which bed rest and treatment by a physician are required.
-
Ratings under diagnostic codes 9201 to 9440 will be evaluated using the General Rating Formula for Mental Disorders. Ratings under diagnostic codes 9520 and 9521 will be evaluated using the General Rating Formula for Eating Disorders.
-
Review the special provisions outlined in 38 CFR 4.125 through 38 CFR 4.129 for decisions related to mental disorders
-
The nomenclature employed in this portion of the rating schedule is based upon the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM–5) (see 38 CFR 4.125 for availability information). Rating agencies must be thoroughly familiar with this manual to properly implement the directives in 38 CFR 4.125 through 38 CFR 4.129 and to apply the general rating formula for mental disorders in 38 CFR 4.130.