9411 - Posttraumatic stress disorder
DBQ: Link to Index of DBQ/Exams by Disability for DC 9411
Acronym: PTSD
Definition
A disorder in which an overwhelming traumatic event is re-experienced, causing intense fear, helplessness, horror, and avoidance of stimuli associated with the trauma.
{kind=link}
It is important to remember that the reaction to stress is highly individualized, and, because of that, the stress that would cause this syndrome in one individual might have little if any effect on another. Prevalence appears to be higher in those considered more at risk, such as combat veterans or victims of criminal violence. The prevalence in these groups is reported to be between 3 and 58%.
Etiology
The development of symptoms usually occurs after a psychologically traumatic event (stressor) that the person experienced, witnessed, or was confronted with that involved actual or threatened death or serious injury, or a threat to the physical integrity of themselves or others.
The following are the main types of PTSD claims* and associated stressors:
-
Combat: A claim for PTSD where the claimed stressor is related to combat. (The decorations identified in M21-1MR IV.ii.1.D.13.d may serve as evidence that the veteran engaged in combat.)
-
Personal Assault: A claim for PTSD where the claimed stressor is related to an event of human design that threatens or inflicts harm. Examples of personal assault stressors may include sexual assault, physical assault, mugging, stalking, sexual harassment, domestic battery, or robbery. Military Sexual Trauma (MST) is the term that VA uses to refer to sexual assault or repeated, threatening sexual harassment that occurred while the Veteran was in the military.
-
Noncombat: A claim for PTSD involving a stressor other than combat or a personal assault. Examples of noncombat stressors may include vehicle accidents, disasters, or perhaps duty on a burn ward or in a graves registration unit.
*Note that 38 C.F.R. 3.304(f)(2) also refers to prisoner of war (POW) experiences as a PTSD stressor.
Signs & Symptoms
The following specifiers are useful in determining the beginning and extent of symptoms:
{kind=link}
-
Acute - Length of symptoms is usually less than 3 months
-
Chronic - Symptoms usually last 3 months or more
-
With delayed onset - Usually at least 6 months have passed between the traumatic experience and the beginning of symptoms
The symptoms may include: recurrent experiences of a traumatic event, avoiding an excitant or irritant associated with the trauma, deadening of general responsiveness, experiencing symptoms related to increased arousal, including insomnia, recurrent nightmares, and extreme caution; exhibiting an inflated frightened response; and experiencing changes in hostility.
Tests
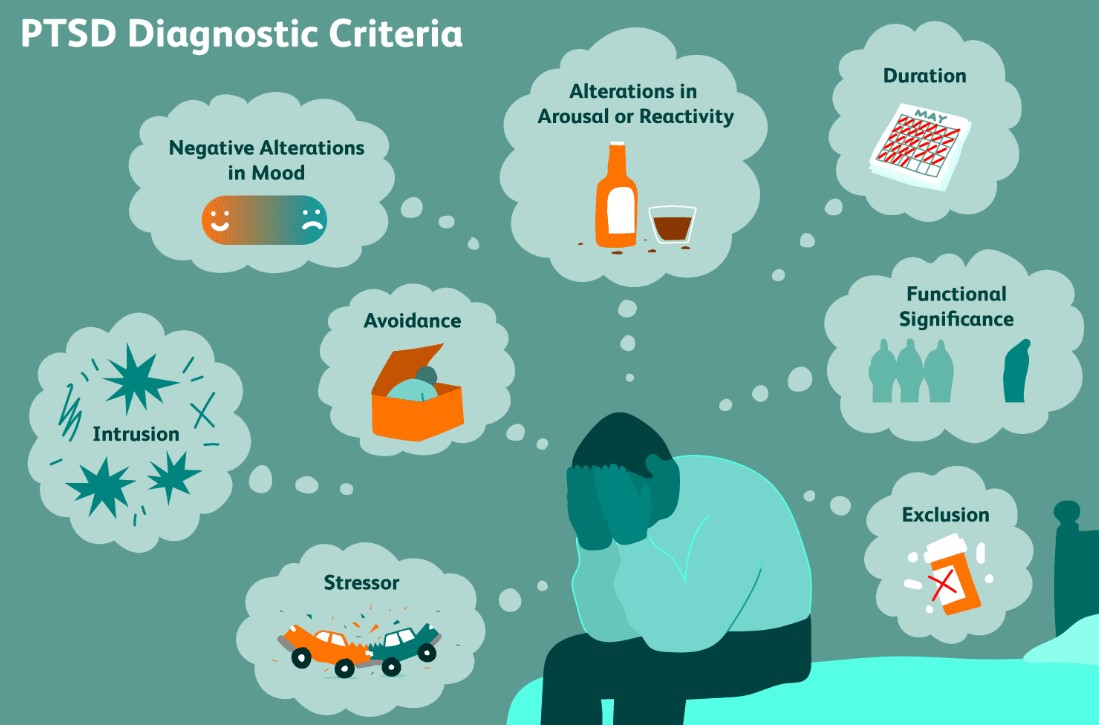
Diagnostic criteria for post-traumatic stress disorder (PSTD) include:
{kind=link}
-
The person has experienced a traumatic event in which both of the following were present:
-
The person had an actual experience, was a witness to, or was confronted with an event or events that concerned actual or threatened death or serious injury, or danger to the physical being of self or others
-
The person's reaction included extreme fear, helplessness, or terror.
-
-
The traumatic event consistently re-occurs in one or more of the following ways:
-
Repeated and disturbing stressful recollections of the event including images, beliefs, or observations
-
Repeated and disturbing stressful dreams of the event
-
Acting or feeling that the event were repeatedly occurring, (e.g., feeling of reliving the experience, delusions, hallucinations, and flashback episodes)
-
Extreme psychological distress experienced when something triggers the thought of the event, e.g., prompts that represent or resemble an aspect of the event
-
Physiologic acts that occur in reaction to exposure to inner or outside stimuli that represent or resemble an aspect of the event.
-
-
Consistent avoidance of stimuli related to the traumatic event and deadening of general responsiveness that was not present before the trauma as indicated by:
-
The taking of measures to avoid beliefs, feelings, or discussions related to the traumatic event
-
The taking of measures to avoid acts, locations, or other persons that stimulate memory of the traumatic event
-
Inability to recall a significant aspect of the trauma
-
Lack of interest in activities or partaking in them or both
-
Feeling of isolation or detachment from others
-
Constrained effect resulting in inability to experience certain feelings, e.g., loving feelings
-
Impression that life may be shortened; lacking expectations regarding the future.
-
-
Consistent indications of arousal that were not present before the traumatic incident, as suggested by the at least two of the following:
-
Inability to fall or stay asleep
-
Irritability or eruptions of anger
-
Problems with concentration
-
Exaggerated frightened reaction
-
Experiences the symptoms listed in criteria b, c, and d for more than one month
-
The disorder causes considerable clinical distress or impaired performance related to social, occupation, or other significant areas of functioning.
-
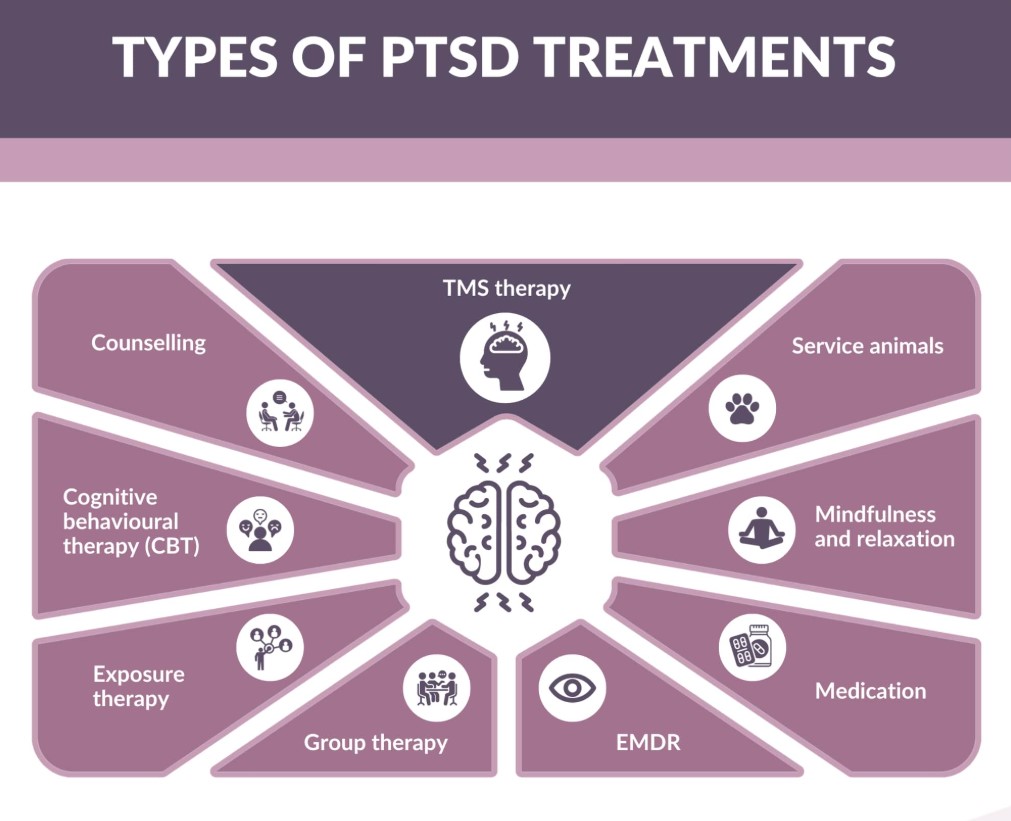
Treatment
Treatment may consist of behavior therapy, medications and psychotherapy. Antidepressant and anti-anxiety drugs appear to have some benefit, but are generally less effective than for other anxiety disorders. In addition, sustained use of these medications may cause physical dependence. Certain medications that inhibit serotonin re-uptake appear to be most effective. Usually the anxiety associated with the traumatic memories is so concentrated that supportive psychotherapy plays a significant role in treatment. In addition, patients may experience guilt because their behavior was aggressive and destructive during armed combat, or "survivor guilt" because they survived a traumatic experience in which significant others or close associates died, resulting in the need for insight-oriented therapy.
{kind=link}
A behavioral therapy called exposure therapy has been found to be one of the most effective treatments for PTSD. This therapy encourages the patient to cease avoidance behaviors through stepwise focusing on the traumatic event and confronting and connecting with feared situations, thoughts, and feelings.
Residuals
It is possible for the disorder to continue for decades. It is estimated that 15% of male and 9% of female Vietnam combat veterans may experience PTSD.
Special Considerations
-
If a Veteran is a former prisoner of war, this disease shall be service connected if manifest to a degree of disability of 10% or more at any time after discharge or release from active military, naval, or air service even though there is no record of such disease during service, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied [38 CFR 3.309 (c) Disease subject to presumptive service connection].
-
May be entitled to special monthly compensation where the Veteran has a single service-connected disability rated as 100% with additional service-connected disability or disabilities independently ratable at 60% or more, which are separate and distinct from the 100% service-connected disability and involves different anatomical segments or bodily systems. See 38 CFR 3.350(i)(1) – Special Monthly Compensation (SMC).
-
Competency must be addressed in cases where a mental condition is initially evaluated as totally disabling or when the total evaluation is continued in a rating decision. This includes when individual unemployability is awarded or continued on the basis of a single mental health disability, and when assigning or continuing a temporary total evaluation for a mental disorder under 38 CFR 4.29 [38 CFR 3.353 [Determinations of incompetency and competency]].”
-
Review 38 CFR 3.354 with regard to determinations of insanity.
-
Reference 38 CFR 3.384 for the applicability of the term psychosis
-
When considering previously denied claims, note that fear based criteria were added to the CFR effective July 13, 2010
-
Reference 38 CFR 3.304(f) relating to principles of service connection for posttraumatic stress disorder (PTSD)
Notes
-
An incapacitating episode is a period during which bed rest and treatment by a physician are required.
-
Ratings under diagnostic codes 9201 to 9440 will be evaluated using the General Rating Formula for Mental Disorders. Ratings under diagnostic codes 9520 and 9521 will be evaluated using the General Rating Formula for Eating Disorders.
-
Review the special provisions outlined in 38 CFR 4.125 through 38 CFR 4.129 for decisions related to mental disorders
-
The nomenclature employed in this portion of the rating schedule is based upon the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM–5) (see 38 CFR 4.125 for availability information). Rating agencies must be thoroughly familiar with this manual to properly implement the directives in 38 CFR 4.125 through 38 CFR 4.129 and to apply the general rating formula for mental disorders in 38 CFR 4.130.