7718 - Essential thrombocythemia and primary myelofibrosis
DBQ: Link to Index of DBQ/Exams by Disability for DC 7718
Definition
Essential thrombocythemia and primary myelofibrosis are two types of chronic myeloproliferative disorders. Essential thrombocythemia is a condition in which the body produces too many platelet cells.
{kind=link}
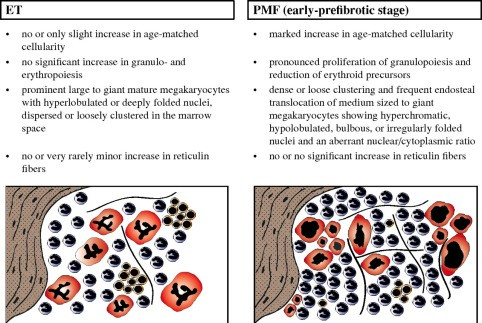
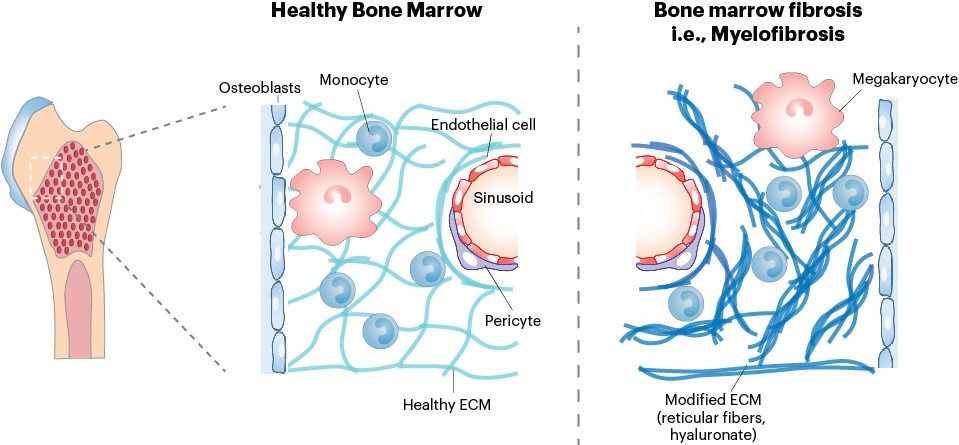
Primary myelofibrosis is a condition in which there is a buildup of scar tissue (fibrosis) in the bone marrow. Because of the fibrosis, bone marrow is unable to make enough normal blood cells.
{kind=link}
Etiology
While there is no definitive cause of essential thrombocythemia, the majority of individuals with the condition have an acquired gene mutation contributing to the disease.
Primary myelofibrosis is thought to be caused by a genetic mutation in the blood stem cells. As the mutated cells replicate and divide, the mutation continues to be passed along and eventually has a serious effect on blood production. This condition is more commonly diagnosed among those aged 50-80 years old.
{kind=link}
Signs & Symptoms
Signs and symptoms of essential thrombocythemia are unnoticeable when the platelet count first increases. Symptoms are varied and include:
-
weakness
-
bruising and bleeding
-
gout
-
paresthesias of the hands and feet
-
thrombotic events.
{kind=link}
Thrombosis may cause symptoms in the affected site, such as:
-
neurologic deficits with stroke or transient ischemic attack
-
leg pain, swelling, or both with lower extremity thrombosis
-
chest pain and dyspnea with pulmonary embolism
Signs and symptoms of primary myelofibrosis depend on the type of cell whose production is reduced. Reduction in red blood cells can cause fatigue and shortness of breath; a shortage in white blood cells can lead to an increased number of infections; and a shortage in platelets can cause easy bruising or bleeding.
Tests
Procedures and tests to diagnose these conditions include:
-
physical exam
-
blood tests (visual inspection, complete blood count (CBC)) with blood smear
-
imaging tests, such as x-rays and magnetic resonance imaging (MRI)
-
bone marrow examination (bone marrow biopsy and/or aspiration)
-
genetic testing
In essential thrombocythemia, samples of blood will be checked for the number of, size, and activity of platelets. Iron levels and markers of inflammation will also be checked. Ruling out causes of secondary thrombocythemia and cytogenetic studies may be completed.
In primary myelofibrosis, the CBC may show abnormally low red blood cell counts, higher than normal white blood cell counts, and either higher or lower platelet counts.
Treatment
Common treatment for essential thrombocythemia includes aspirin and platelet-lowering drugs. In rare cases, treatment includes plateletpheresis, chemotherapy, interferon, and stem cell transplantation.
Treatment for primary myelofibrosis is directed at symptoms and complications. Treatment includes symptomatic therapy, allogeneic stem cell transplantation, and chemotherapy.
Residuals
Individuals with essential thrombocythemia can live long lives. Although symptoms are common, the course of the disease is usually benign. Serious arterial and venous thrombotic complications are rare, but can be life-threatening. In rare cases, the disease can transform into primary myelofibrosis or acute myeloid leukemia.
Special Considerations
-
Prior to December 9, 2018, this condition was evaluated analogously to Hodgkin's lymphoma (7799-7709) (previously Hodgkin's disease).
-
Rate a solitary plasmacytoma that has developed into multiple myeloma as symptomatic multiple myeloma.
-
Rate residuals of plasma cell dysplasia (e.g., thrombosis) and adverse effects of medical treatment (e.g., neuropathy) under the appropriate diagnostic codes.
Notes
-
If the condition undergoes leukemic transformation, evaluate as leukemia under diagnostic code 7703.
-
A 100 percent evaluation shall be assigned as of the date of hospital admission for peripheral blood or bone marrow stem cell transplant; or during the period of treatment with chemotherapy (including myelosuppressants) or interferon treatment. Six months following hospital discharge or, in the case of chemotherapy treatment, six months after completion of treatment, the appropriate disability rating shall be determined by mandatory VA examination. Any reduction in evaluation based upon that or any subsequent examination shall be subject to the provisions of 38 CFR 3.105(e).