7712 - Multiple myeloma
DBQ: Link to Index of DBQ/Exams by Disability for DC 7712
Acronym: MM
Definition
Asymptomatic myeloma (smoldering or indolent) is a slow-growing, asymptomatic precursor or pre-malignant phase of multiple myeloma. This type of myeloma is a condition between monoclonal gammopathy of undetermined significance (MGUS) and active multiple myeloma.
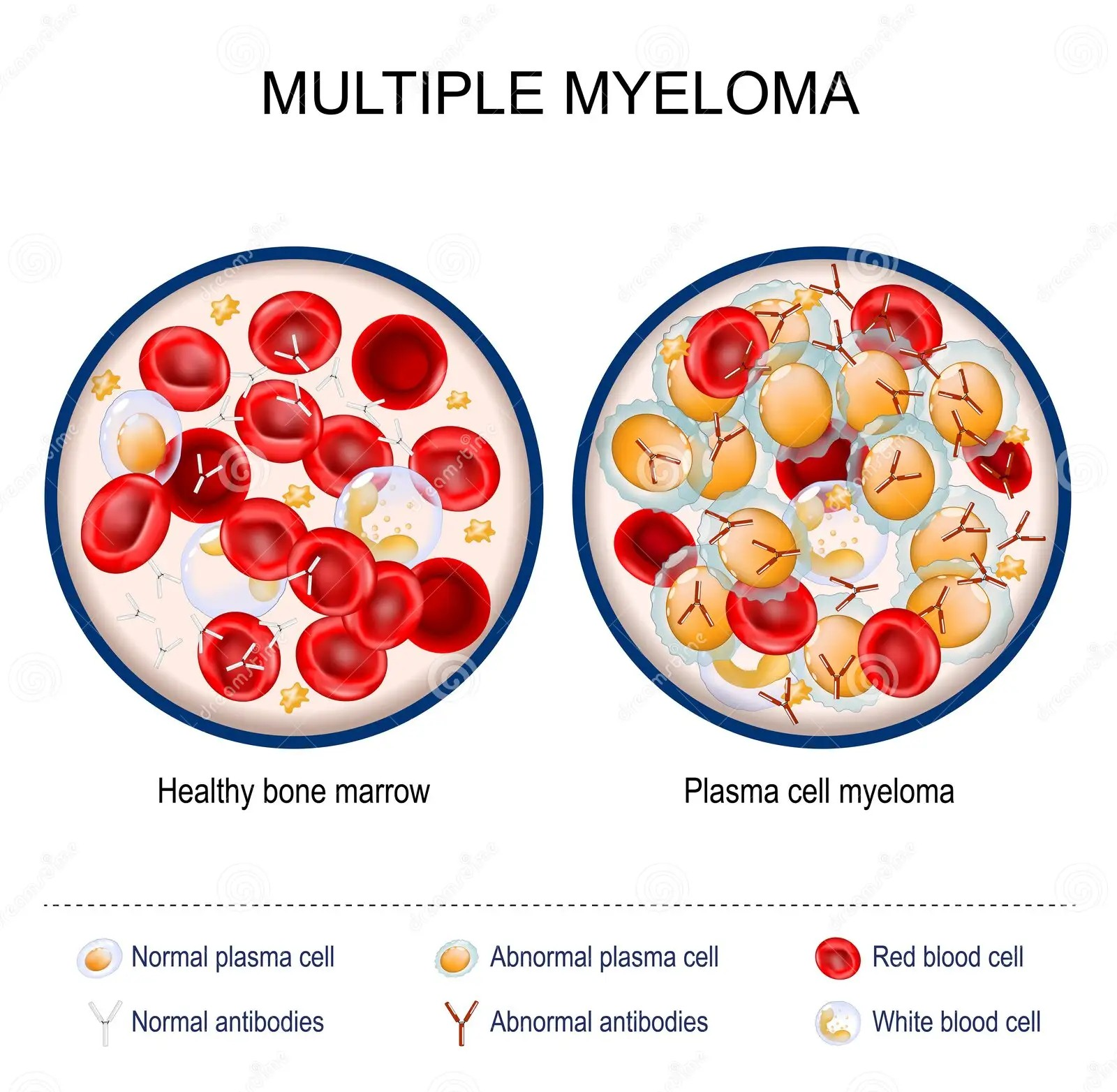
Multiple myeloma is a cancer of the plasma cells in the bone marrow. These cells produce excessive levels of monoclonal immunoglobulin, antibodies that are normally made by plasma cells to recognize antigens and fight infection. Multiple myeloma is also referred to as malignant plasmacytoma, plasma cell dyscrasia, plasma cell myeloma and plasmacytoma of bone.
{kind=link}
Etiology
Multiple myeloma is characterized by the excessive growth and malfunction of plasma cells in the bone marrow. The growth of these extra plasma cells interferes with the production of red blood cells, white blood cells, and platelets. They infiltrate virtually all of a patient's bone marrow. Multiple myeloma is not confined to a specific bone or location within a bone. It tends to involve the entire skeleton. When only one lesion is found, it is called a plasmacytoma. Multiple myeloma occurs spontaneously. Patients exposed to ionizing radiation and pesticide dioxin may develop the disease. Infection with some viruses such as HIV and human herpes has also been associated with multiple myeloma.
Multiple myeloma mainly affects older adults and tends to be more common in men and twice as common in African Americans as it is in Caucasians. There are no known inherited risk factors. Other risk factors are unknown.
Signs & Symptoms
Asymptomatic myeloma (smoldering or indolent) is not usually treated until evidence of end organ damage develops and it has a high risk of developing into multiple myeloma. About 50 percent of those diagnosed with the condition will develop multiple myeloma within five years.
Even if smoldering multiple myeloma is currently regarded as a pre-malignant state, there are subsets of patients with different rates of progression towards multiple myeloma. No single pathological or molecular feature can be used to distinguish between smoldering and pre-malignant multiple myeloma with clonal plasma cells from those with clonal malignant plasma cells. A biomarker-based definition that can predict this transformation is needed but is not yet currently available.
Symptomatic multiple myeloma causes the following:
-
bone pain/tenderness, usually in the back, pelvis, sternum, or ribs
-
fevers
-
night sweats
-
unexplained or pathogenic fractures due to destruction of the bones
-
bleeding problems
-
increased susceptibility to infection
-
nausea
-
confusion
-
constipation
-
frequent urination
-
symptoms of anemia, such as tiredness, weakness, shortness of breath, and fatigue
-
numbness or paralysis due to compression of the nerves (if bones/spine are affected)
-
renal failure
-
leukopenia
-
thrombocytopenia
-
hypercalcemia.
Tests
Tests will include the following:
-
a complete history and physical examination for early diagnosis and treatment
-
computed tomography (CT) scan
-
magnetic resonance imaging (MRI)
-
needle biopsy of the bony lesion and regional lymph nodes
-
histological studies of bone marrow
-
complete blood count (CBC)
-
urinalysis
-
a chemistry profile.
A bone scan may show which bones are involved with multiple myeloma, but often the lesions cannot be seen. Multiple myeloma appears on X-rays as decreased bone density with many holes in the bone (destructive lesions). Additional tests may be conducted to determine if the cancer has involved other parts of the skeleton or other sites such as the lungs, and to determine staging of the disease. Diagnosis is made when a large number of abnormal plasma cells are found in the patient's bone marrow.
Treatment
Asymptomatic myeloma (smoldering or indolent) is not malignant and does not require treatment.
Multiple myeloma is currently not curable. The standard treatment with medications is melphalan and prednisone. These treatments may cause severe muscle weakness and may increase the chance of infections. Radiation therapy is reserved for decreasing the size of symptomatic bone lesions. A recent advancement in the treatment of multiple myeloma has increased response rates and survival. The treatment consists of high dose chemotherapy followed by autologous stem cell transplantation. This treatment may decrease symptoms and prolong life expectancy, giving patients a 20 percent chance of living longer than 10 years. Bone marrow transplantation (BMT) and peripheral blood stem cell transplantation (PBSCT) are procedures that restore stem cells that were destroyed by high doses of chemotherapy and/or radiation therapy. BMT and PBSCT may extend remission rather than provide a cure.
Bisphosphonates are used to prevent destructive bone lesions and spine fractures. Erythropoietin or occasional blood transfusions are used to manage anemia. Antibody infusions and vaccinations may be used to help patients with recurrent infections. Corticosteroids and hydration may be used to treat high blood calcium concentrations (from bone loss) and dehydration. Narcotics can address the pain associated with bone lesions. Operative intervention may be required to control the pain associated with bone fractures. The goal of treatment is to relieve symptoms. Chemotherapy and transplant rarely lead to permanent cure. Supportive care includes comfort measures, pain control and interventions that maintain function.
Additionally, managing the bone disease, anemia, infections, kidney failure and pain associated with multiple myeloma are included in the supportive care regimen. Individuals who have mild disease, or in whom the diagnosis is uncertain are usually monitored without treatment. Some people have a slow-developing form of multiple myeloma, which takes years before it causes symptoms. When the disease advances or causes symptoms, treatment is implemented.
Residuals
Residual effects of multiple myeloma coincide with unwanted side effects of chemotherapy, stem cell transplantation, and radiation. Side effects may depend on the type and extent of the treatment and may vary for each person, as well as change from one treatment session to the next. Other health problems may arise from the condition and its treatments. These may include infection, anemia, pain, thinning bones, hypercalcemia, alteration in kidney function, and amyloidosis. Nutritional deficits may also become problematic as a result of treatment side effects that cause poor appetite, nausea, vomiting, or mouth sores.
Special Considerations
-
Prior to December 9, 2018, this condition was evaluated analogously to Hodgkin's lymphoma ((7799-7709) (previously Hodgkin's disease)).
-
Prior to December 9, 2018, multiple myeloma was assigned a permanent and total (P&T) evaluation based on diagnosis alone. Following this date (the date the rating schedule was updated), this is no longer the case. Refer to the M21 for more information.
-
Consider service connection on a presumptive basis as a condition associated with ionizing radiation exposure (38 CFR 3.307; §3.309(d); §3.311).
-
Consider service connection on a presumptive basis as a condition associated with herbicide exposure (38 CFR 3.307(a)(6); §3.307(d); §3.309(e)).
-
Consider service connection on a presumptive basis as a condition associated with exposure to contaminated water at Camp Lejeune (38 CFR 3.307(a)(7); §3.307(d); §3.309(f)).
Notes
-
Current validated biomarkers of symptomatic multiple myeloma and asymptomatic multiple myeloma, smoldering, or monoclonal gammopathy of undetermined significance (MGUS) are acceptable for the diagnosis of multiple myeloma as defined by the American Society of Hematology (ASH) and International Myeloma Working Group (IMWG).
-
The 100 percent evaluation shall continue for five years after the diagnosis of symptomatic multiple myeloma, at which time the appropriate disability evaluation shall be determined by mandatory VA examination. Any reduction in evaluation based upon that or any subsequent examination shall be subject to the provisions of 38 CFR 3.105(e) and §3.344(a) and (b).