7535 - Toxic nephropathy (antibotics, radiocontrast agents, nonsteroidal anti-inflammatory agents, heavy metals, and similar agents)
DBQ: Link to Index of DBQ/Exams by Disability for DC 7535
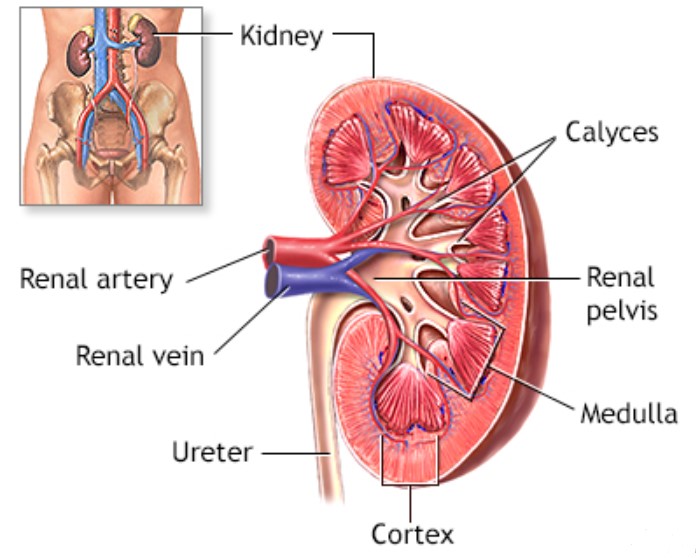
Definition
Toxic nephropathy of the kidney refers to a change in the structure or action performed by the kidney resulting from ingestion, injection, inhalation or absorption of a chemical or biologic agent.
{kind=link}
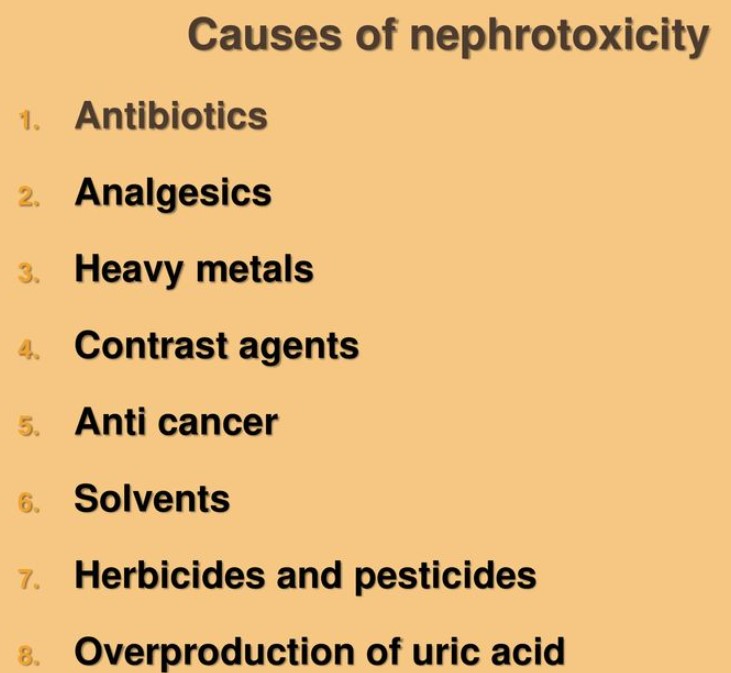
Etiology
Antibiotics are the leading cause of nephrotoxicity. Other causes may include: electrolyte imbalances such as hypokalemia, hyperkalemia, hypomagnesemia, or hyperuricemia; contrast agents used for radiography studies; and analgesics such as aspirin and nonsteroidal anti-inflammatory drugs (NSAID). In addition, impaired arterial circulation and immunologic injury may cause this condition. Additional causes include: heavy metal accumulation, such as from industrial exposure; contaminated water; wine or alcohol; mining; smoke inhalation; leaded gasoline; or iron overload. Environmental agents such as solvents or pesticides, and agents used in chemical warfare are etiologic factors. Use of unregulated foods, herbs, and plant medicines; and contact with poison ivy or oak and certain fungi may also cause nephrotoxicity.
{kind=link}
{kind=link}
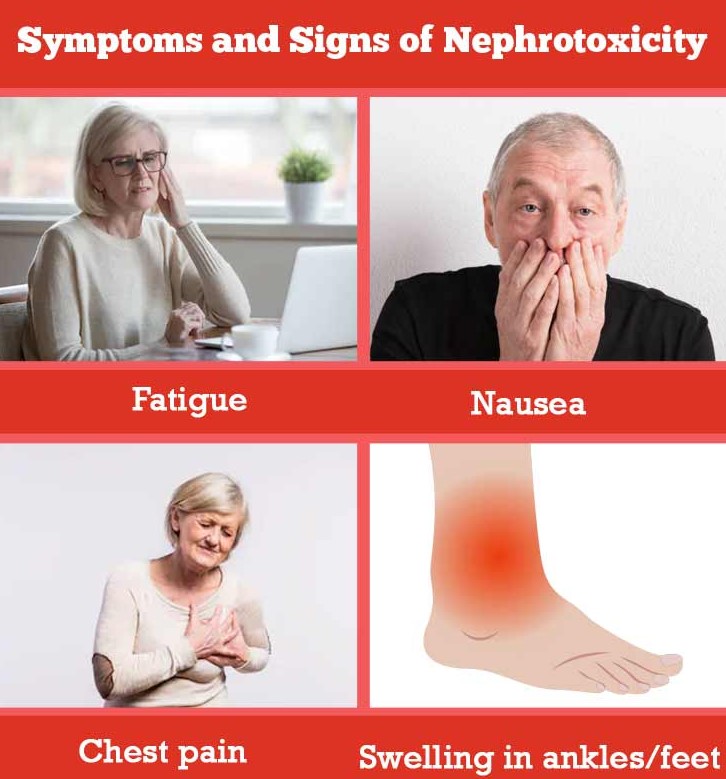
Signs & Symptoms
Signs and symptoms may depend on the causative agent, the degree of loss of excretory function, and the degree and rate of renal failure. Manifestations related to these conditions may include those of acute and chronic renal failure (see Diagnostic Code: 7530 Chronic renal disease requiring regular dialysis). Manifestations of the acute and chronic conditions include: nephrotic syndrome; tubular acidosis; and tubulointerstitial nephritis. Other signs and symptoms of these conditions may be cola-colored urine; diminished urination (oliguria); absence of urine formation (anuria); protein in the urine (proteinuria); frothy urine; generalized edema; ascites; pleural effusion; chest pain; cardiac arrhythmias; blood pressure changes; loss of appetite (anorexia); malaise; decreased reflexes; and paralysis. In addition, there may be other manifestations including: abdominal pain; retinal sheen; muscle atrophy; lipiduria; lipemia; fever; infection; thrombosis; urticarial rash; abnormal urinalysis and blood studies; excessive urination (polyuria); metabolic acidosis; osteopenia; bone pain; and renal calculi.
{kind=link}
{kind=link}
Tests
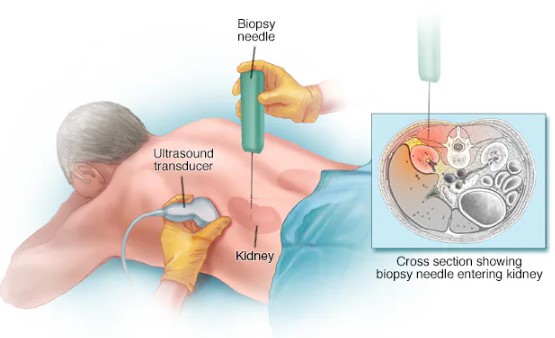
Diagnostic measures may include: urine and blood chemistry analyses; urine and blood cultures; drug screens; x-ray; ultrasonography; computed tomography (CT) scan; magnetic resonance imaging (MRI); renal arteriography or venography; and renal biopsy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment
Treatment may depend on the underlying cause which may include: removing the toxic agent by vomiting (emesis); enhanced diuresis; hemodialysis; or a combination of these measures. There may be a need to treat acidosis in certain conditions. Other treatments consist of restricting fluid intake; low-protein diet; monitoring body weight; multivitamins; anticoagulants; antibiotic therapy; antioxidants; and sodium bicarbonate. Respiratory assistance may be needed depending on the type and amount of the circulating toxic agent. Surgical kidney transplantation may be necessary.
Residuals
Patient education related to over-the-counter medications and their side effects may be needed. Some patients, such as those who are over the age of sixty, have conditions such as diabetic neuropathy, myeloma, hyperuricemia, and heart failure, and who have had multiple exposures at frequent intervals, may be predisposed to allergies to radiologic contrast agents. In addition to loss of kidney function, there may be an immunologic deficit. Some toxins may metabolize into neurotoxins and ocular toxins.
Special Considerations
-
This disease, (condition), only in its active form , has a 3 year presumptive period and shall be granted service connection although not otherwise established as incurred in or aggravated by service if manifested to a compensable degree within the applicable time limits under 38 CFR 3.307 following service in a period of war or following peacetime service on or after January 1, 1947, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied. [38 CFR 3.309 [Disease subject to presumptive service connection], 38 CFR 3.309(a). [chronic disease].
-
May be entitled to special monthly compensation where the Veteran has a single service-connected disability rated as 100% with additional service-connected disability or disabilities independently ratable at 60% or more, which are separate and distinct from the 100% service-connected disability and involves different anatomical segments or bodily systems. See 38 CFR 3.350(i)(1) – Special Monthly Compensation (SMC).
-
The new criteria for the Genitourinary Disease and Conditions body system became effective November 14, 2021. Review both current and historic criteria prior to any reduction for disabilities established before that date. 38 CFR 3.951(a)
Notes
-
When evaluating any claim involving loss or loss of use of one or more creative organs, refer to 38 CFR 3.350 of this chapter to determine whether the Veteran may be entitled to special monthly compensation. Footnotes in the schedule indicate conditions which potentially establish entitlement to special monthly compensation; however, there are other conditions in this section which under certain circumstances also establish entitlement to special monthly compensation.
-
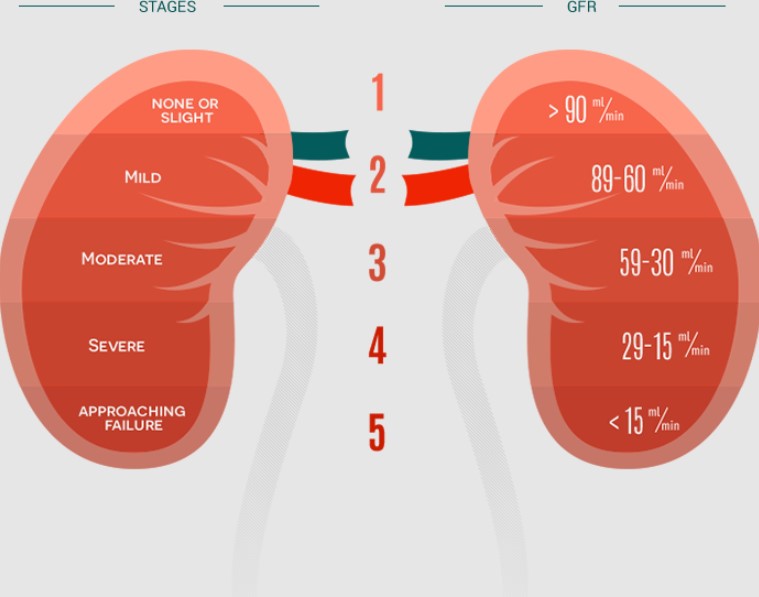
GFR, estimated GFR (eGFR), and creatinine-based approximations of GFR will be accepted for evaluation purposes when determined to be appropriate and calculated by a medical professional.