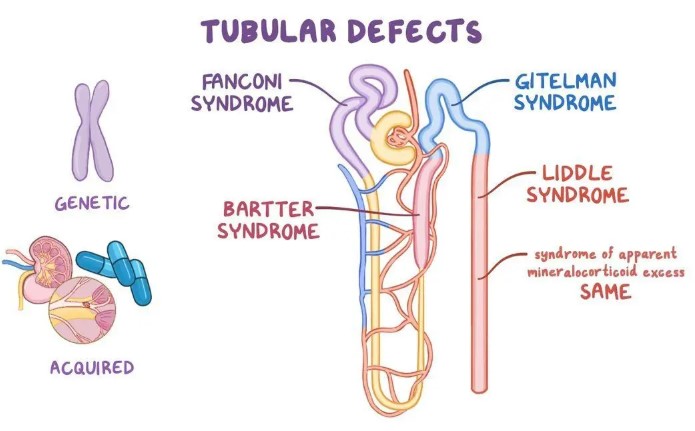
7532 - Renal tubular disorders (such as renal glycosurias, aminoacidurias, renal tubular acidosis, Fanconi's syndrome, Bartter's syndrome, related disorders of Henle's loop and proximal or distal nephron function, etc.)
DBQ: Link to Index of DBQ/Exams by Disability for DC 7532
Definition
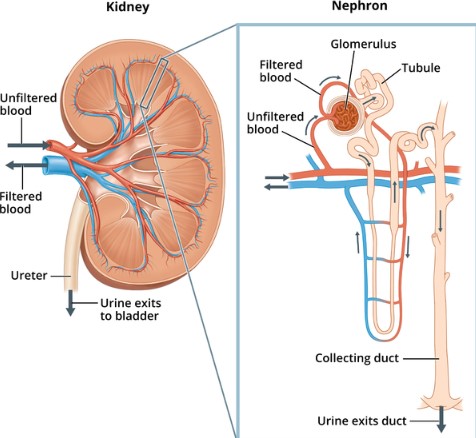
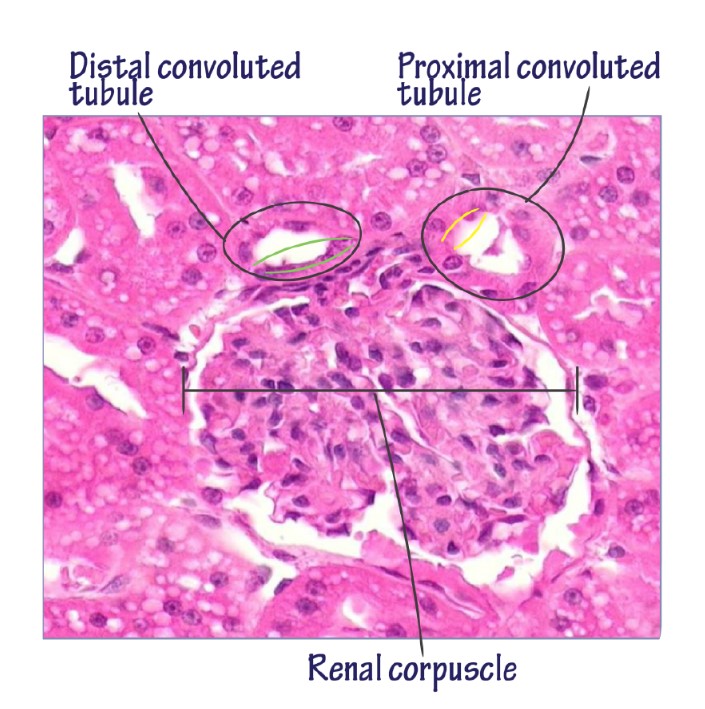
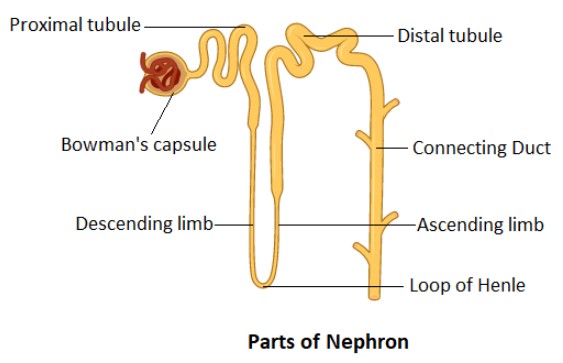
The nephron is the functional unit of the kidney, which includes small, tubular structures. The function of the nephron is to clean and clear the blood plasma of unnecessary material. The blood is then filtered by the glomerulus, and is then separated in the tubules as necessary and unnecessary fluids. The necessary fluids are returned to the blood stream, and the unnecessary ones are excreted as urine. The entire tubule is made up by three sections: the proximal convoluted tubule, Henle's loop, and the distal convoluted tubule. Urine is formed in the renal corpuscles by filtration, reabsorption and emission from the cells of the renal tubule sections (see below).
{kind=link}
-
Proximal convoluted tubules - The majority of electrolytes are reabsorbed here via active transport. Hydrogen ions and creatinine are emitted into the filtrate.
-
Henle's loop - Reabsorption continues here. Water is conserved, thus concentrating the filtrate. Approximately one -quarter of filtered sodium is reabsorbed here.
-
Distal convoluted tubules - Provides for the final regulation of water and acid-base balance. The release of antidiuretic hormone (ADH) provides for greater permeability of this area to water.
{kind=link}
{kind=link}
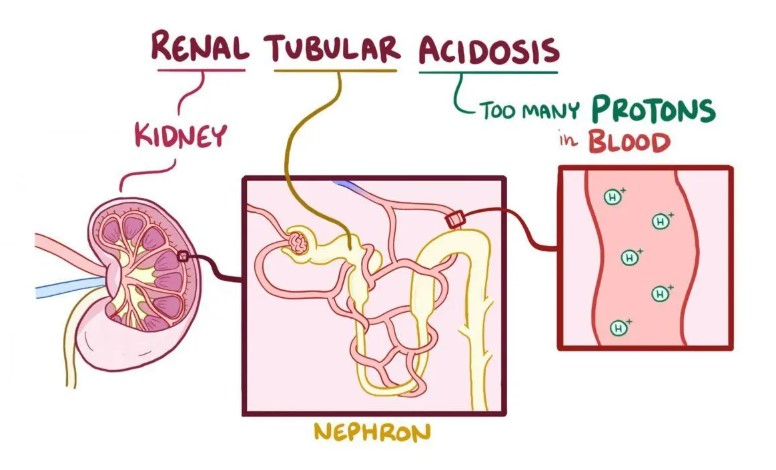
There are four types of renal tubular acidosis. Types I (distal) and II (proximal) are usually hereditary. Type III is rare, and is a combination of types I and II. Type IV is acquired. Other selected tubular disorders include: Fanconi's syndrome, aminoaciduria, and glucosuria.
{kind=link}
Etiology
Etiologies include, but are not limited to: heredity (types I and II); diabetes mellitus; toxins (heavy metals, lead); sickle cell disease; stomach lupus; hyperparathyroidism; and renal transplant.
{kind=link}
Signs & Symptoms
Manifestations of types of renal tubular disorders are as follows:
-
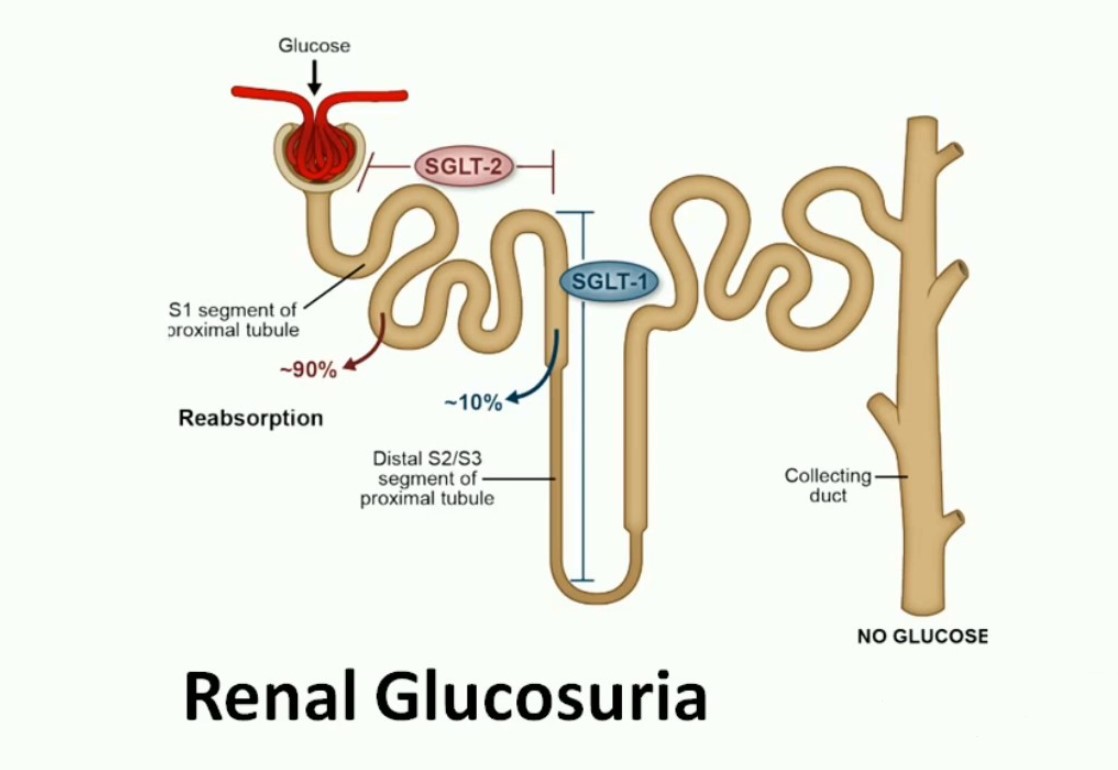
Glucosuria - Excretion of glucose in the urine with no apparent symptoms.
-
Aminoaciduria - Sustained levels of excess amino acids in the urine may cause several problems including: mental deficiency; severe brain damage; phenylketonuria; and ketosis.
-
Renal tubular acidosis - Type I classification causes excessive calcium in the urine (hypercalciuria), calcium stones, and deposits of calcium in the renal tubules (nephrocalcinosis). Adults with this condition develop softening of the bones (osteomalacia). Type II classification may cause only temporary proximal tubular dysfunction. Type IV classification is usually associated with decreased aldosterone in the blood (hypoaldosteronism) secondary to diabetic nephropathy. Hypertension results in nephrosclerosis. In addition, these patients have high serum potassium levels and low urine ammonia excretion. Renal calculi are not presented.
-
Fanconi's syndrome - Adults develop laboratory abnormalities of renal tubular acidosis; decreased levels of phosphate in the blood (hypophosphatemia); and low potassium blood levels (hypokalemia). In addition, symptoms of bone disease (osteomalacia) and muscle weakness may occur.
{kind=link}
{kind=link}
Tests
Diagnostic measures related to types of renal tubular disorders are as follows:
-
Glucosuria - Blood glucose levels go beyond the renal threshold (approximately 170 mg/dL) in a regular urinalysis, or the demonstration of glucose in the blood after an overnight fast (fasting glucose).
-
Aminoaciduria - A urine specimen is obtained to evaluate for the presence of amino acids. Normal value range depends on the age of the patient.
-
Renal tubular acidosis - Laboratory tests are conducted to determine the presence of the following: hypercalciuria; nephrocalcinosis; hypoaldosteronism; increased potassium level (hyperkalemia); and decreased ammonia levels.
-
Fanconi's syndrome - Diagnosis is confirmed by the determination that abnormalities of renal function exist, especially when glucose, phosphate and amino acids are present in the urine.
{kind=link}
{kind=link}
Treatment
Measures of treatment related to types of renal tubular disorders are as follows:
-
Glucosuria - No treatment is necessary.
-
Aminoaciduria - Disorders of amino transport may occur secondary to several causes and may involve several different amino acids. The presence of cystine in the urine (cystinuria) is the most common amino acid transport dysfunction. The aim of treatment is to avoid cystine crystal development by reducing the amount of cystine in the urine. This is accomplished by increasing the volume of urine and sustaining alkaline urine.
-
Renal tubular acidosis - Sodium bicarbonate alleviates symptoms and averts or stabilizes renal failure and bone disease. Other electrolytes are replaced as indicated.
-
Fanconi's syndrome - There is no specific treatment unless removing the offending toxin is appropriate. However, sodium bicarbonate or other solutions that are better tolerated may be given to decrease the acidosis. In addition, potassium supplements may be given when indicated.
Residuals
Residuals related to types of renal tubular disorders are as follows:
-
Glucosuria - Glucosuria occurs without symptoms or serious continuation. A small number of patients develop diabetes mellitus. However, this may be discounted by determining the cause of glucosuria.
-
Aminoaciduria - Management with fluids and medications is indicated first. However, some of the medications given may cause additional problems, e.g., the constant administration of sodium bicarbonate to maintain alkalinity may result in the formation of a different composition of stones. In addition, the administration of medications that lower cystine levels, may cause other serious illness, and are reserved for high-risk conditions. If medical treatment fails, surgery is indicated as a last resort since cystine stones reform more easily in scar tissue.
-
Renal tubular acidosis - Renal calculi may form if acidosis is not reduced. Patients will remain on medications to maintain potassium levels, and will be placed on low-potassium diets.
-
Fanconi's syndrome - If renal failure occurs, renal transplantation is indicated. The surgery has been successful. However, if cystinosis (abnormal deposits of cystine in body tissues) is the fundamental cause, damage may continue in other organs and ultimately result in death.
Special Considerations
-
May be entitled to special monthly compensation where the Veteran has a single service-connected disability rated as 100% with additional service-connected disability or disabilities independently ratable at 60% or more, which are separate and distinct from the 100% service-connected disability and involves different anatomical segments or bodily systems. See 38 CFR 3.350(i)(1) – Special Monthly Compensation (SMC).
-
The new criteria for the Genitourinary Disease and Conditions body system became effective November 14, 2021. Review both current and historic criteria prior to any reduction for disabilities established before that date. 38 CFR 3.951(a)
Notes
-
When evaluating any claim involving loss or loss of use of one or more creative organs, refer to 38 CFR 3.350 of this chapter to determine whether the Veteran may be entitled to special monthly compensation. Footnotes in the schedule indicate conditions which potentially establish entitlement to special monthly compensation; however, there are other conditions in this section which under certain circumstances also establish entitlement to special monthly compensation.
-
GFR, estimated GFR (eGFR), and creatinine-based approximations of GFR will be accepted for evaluation purposes when determined to be appropriate and calculated by a medical professional.