7530 - Chronic renal disease requiring regular dialysis
DBQ: Link to Index of DBQ/Exams by Disability for DC 7530
Definition
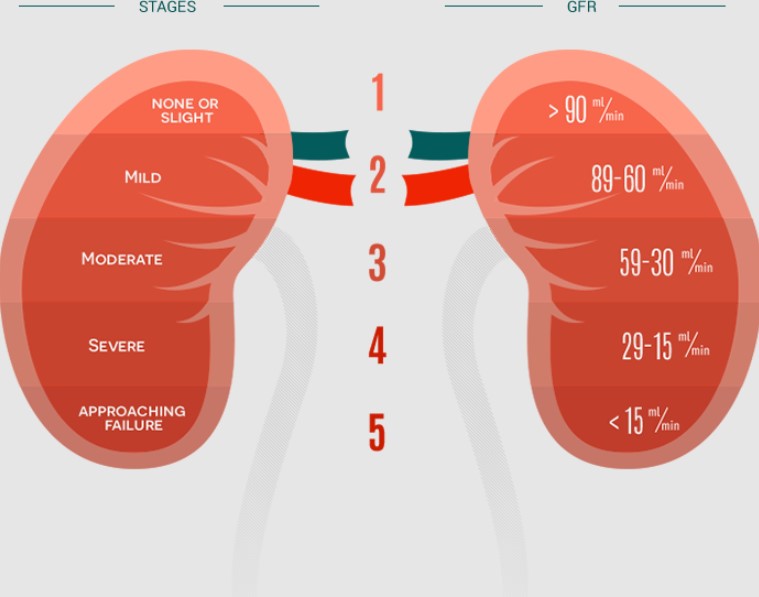
Generally, chronic renal disease is the result of progressive loss of renal (kidney) function. Symptoms usually do not appear until the disease has progressed to the extent that the filtration ability of the kidney has been reduced by 75%.
{kind=link}
Etiology
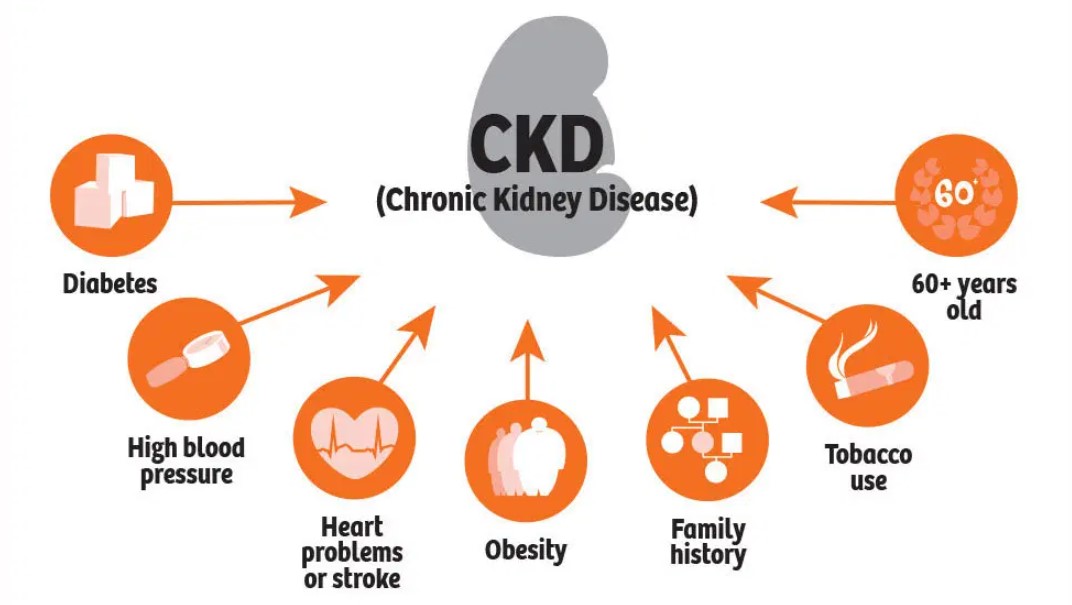
Examples of possible causes of chronic renal disease include the following conditions:
{kind=link}
-
Chronic disease - glomerulonephritis
-
Chronic infections - chronic pyelonephritis or tuberculosis
-
Abnormalities present at birth - polycystic kidney disease
-
Vascular disease - renal nephrosclerosis or hypertension
-
Obstructive processes - calculi
-
Collagen diseases - systemic lupus erythematosus (SLE)
-
Nephrotoxic agents - long-term aminoglycoside therapy
-
Endocrine diseases - diabetic neuropathy
-
Acute renal failure - unresponsiveness to treatment
Signs & Symptoms
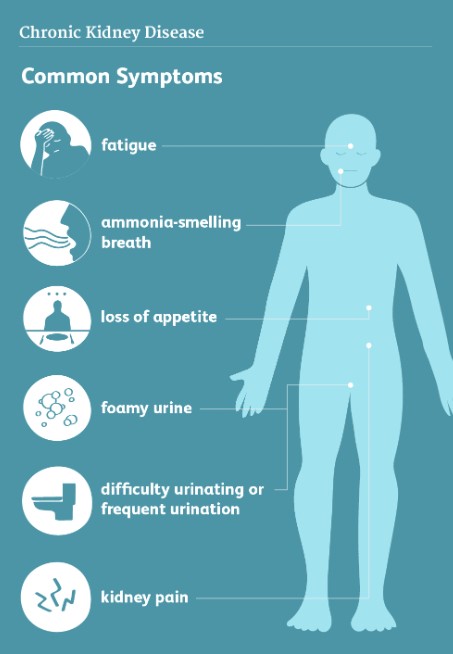
Manifestations of chronic renal disease presented in the following body symptoms are as follows:
{kind=link}
-
Renal and urinary system - Initially, salt-wasting and resulting hyponatremia produce hypotension, dry mouth, skin swelling, fatigue, and nausea. Later, sleepiness/drowsiness and confusion develop. As the number of functioning nephrons decreases, so does the capacity of the kidney to excrete sodium, resulting in salt/sodium retention and overload. Accumulation of potassium causes muscle irritability, and then weakness develops as the potassium level continues to rise. Fluid overload and metabolic acidosis also occur. Urine output decreases and the urine is dilute and contains casts and crystals.
-
Cardiovascular system - Renal failure leads to hypertension; dysrhythmias; cardiomyopathy; uremic pericarditis; pericardial effusion with possible acute compression of the heart; congestive heart failure (CHF); and peripheral swelling.
-
Respiratory system - Changes in the lungs include: reduced pulmonary macrophage, causing increased susceptibility to infection; pulmonary swelling; pleuritic pain; pleural friction rub and effusion; uremic pleuritis and uremic lung or uremic pneumonitis; dyspnea from CHF; and Kussmaul's respiration as a result of acidosis.
-
Gastrointestinal (GI) system - Inflammation and ulceration of the GI mucosa cause stomatitis, gum ulceration and bleeding. In addition, possible manifestations include: parotitis; esophagitis; gastritis; duodenal ulcers; lesions in the small and large bowel; uremic colitis; pancreatitis; and proctitis. Other GI symptoms include a metallic taste in the mouth; ammonia odor to the breath; anorexia; and nausea and vomiting.
-
Skin - Typically, the skin lacks color, and becomes yellowish bronze, dry, and scaly. Other symptoms include: severe itching; purpura ecchymoses; petechiae; uremic frost; thin, brittle fingernails with characteristic lines; and dry, fragile hair that may change color and fall out easily.
-
Neurologic system - Restless leg syndrome may occur as one of the first signs of peripheral neuropathy, causing pain, burning, and itching in the legs and feet. Eventually, this condition progresses to paresthesia and motor nerve dysfunction unless dialysis is initiated. Other signs and symptoms include: muscle cramping and twitching; shortened memory and attention span; apathy; drowsiness; irritability; confusion; coma; and convulsions.
-
Endocrine system - Common abnormalities include: stunted growth patterns in children; infertility; decreased libido in both sexes; amenorrhea; impotence and decreased sperm production in men; increased aldosterone secretion; and impaired carbohydrate metabolism.
-
Hematopoietic system - Common abnormalities include: anemia; decreased red blood cell (RBC) survival time; blood loss from dialysis and GI bleeding; mild thrombocytopenia; and platelet defects. Other problems include: increased bleeding and clotting disorders, demonstrated by purpura; hemorrhage from body orifices; easy bruising; ecchymosis; and petechiae.
-
Musculoskeletal system - Associated abnormalities include: calcium-phosphorus imbalance and resulting parathyroid hormone imbalances, causing muscle and bone pain; skeletal demineralization; pathologic fractures; and calcification in the brain, eyes, gums, joints, myocardium, and blood vessels. Calcification of the arteries may produce coronary artery disease (CAD).
Tests
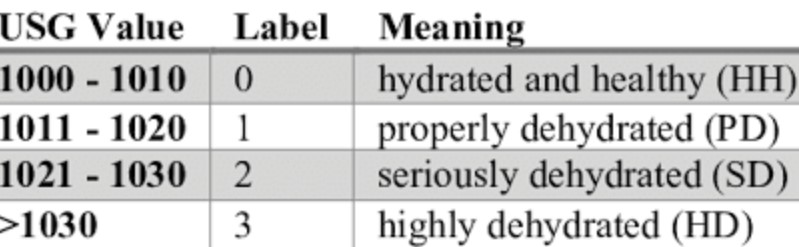
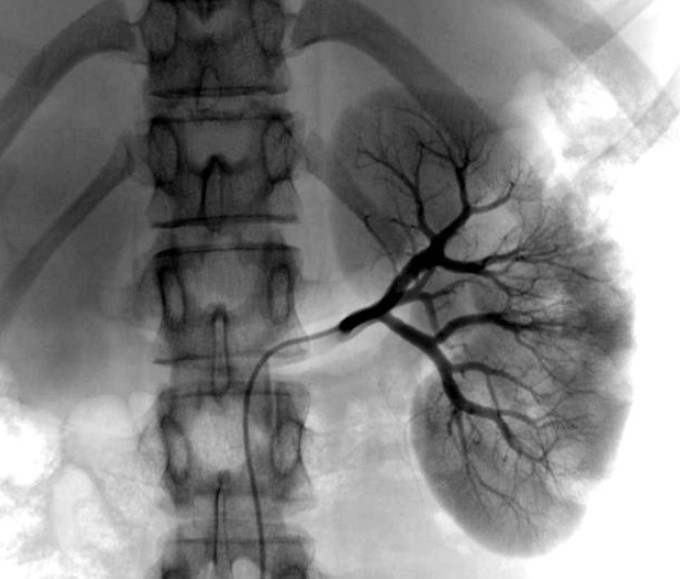
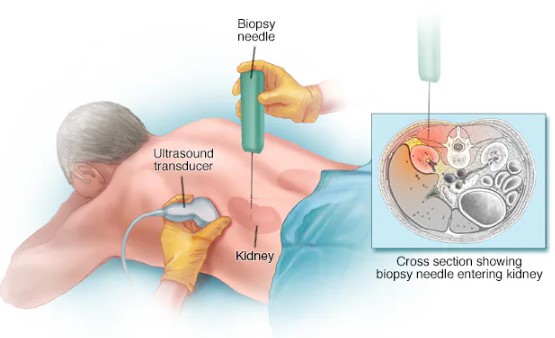
Diagnostic indicators of renal failure include: creatinine clearance tests to identify the stage of chronic renal failure; blood studies that show elevated blood urea nitrogen (BUN), creatinine and potassium levels; decreased arterial pH and bicarbonate levels; and low hemoglobin and hematocrit levels. Urine specific gravity becomes fixed at 1.010, and urinalysis may show proteinuria, glycosuria, erythrocytes, and casts (shed pliable or fibrous material). X-ray studies performed include: kidney, ureter, and bladder film (KUB); intravenous pyelogram (IVP); and a renal scan arteriography (x-ray of arteries after introduction of contrast material). Kidney biopsy may also identify existence of underlying abnormality.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment
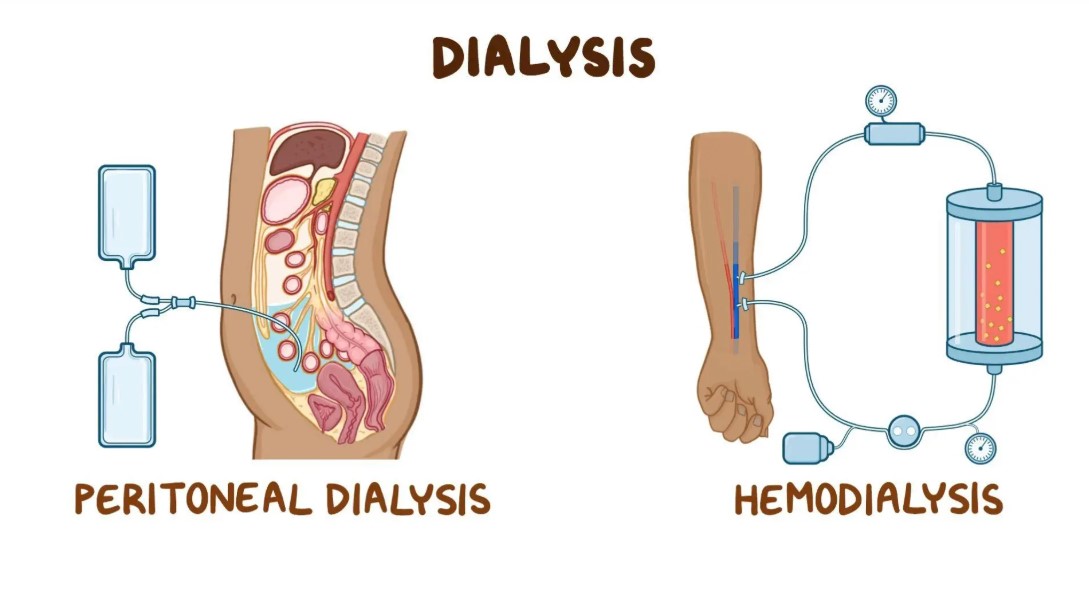
Early in the disease, the goal is to preserve whatever kidney function may be present. Maintenance of fluid balance with diuretics and fluid restriction is essential. Various drugs are used to control swelling, constipation, high blood pressure, nausea, vomiting, gastric irritation, anemia, and itching. Constant laboratory analyses of urine, blood, and stool samples provide information to regulate treatment. As the disease progresses, close monitoring is maintained to determine if dialysis is necessary. Two methods of dialysis may be performed; peritoneal dialysis or hemodialysis.
{kind=link}
Residuals
Complications that may occur from hemodialysis may include, but are not limited to: infection; hemorrhage; stenosis or thrombosis of the venous access; hypotension; arrhythmia; metabolic imbalance; pruritus; insomnia; dementia; and muscle cramps. Complications that may occur from peritoneal dialysis include, but are not limited to: hematoma or abscess at the pericatheter tract; intra-abdominal bleeding; infection; hypotension; catheter obstruction; pneumonia; hyperglycemia; and abdominal and inguinal hernias.
Special Considerations
-
This disease, (condition), only in its active form , has a 3 year presumptive period and shall be granted service connection although not otherwise established as incurred in or aggravated by service if manifested to a compensable degree within the applicable time limits under 38 CFR 3.307 following service in a period of war or following peacetime service on or after January 1, 1947, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied. [38 CFR 3.309 [Disease subject to presumptive service connection], 38 CFR 3.309(a). [chronic disease].
-
May be entitled to special monthly compensation where the Veteran has a single service-connected disability rated as 100% with additional service-connected disability or disabilities independently ratable at 60% or more, which are separate and distinct from the 100% service-connected disability and involves different anatomical segments or bodily systems. See 38 CFR 3.350(i)(1) – Special Monthly Compensation (SMC).
-
The new criteria for the Genitourinary Disease and Conditions body system became effective November 14, 2021. Review both current and historic criteria prior to any reduction for disabilities established before that date. 38 CFR 3.951(a)
-
A report of the Institute of Medicine of the National Academy of Sciences has identified some long-term health effects, listed in the table embedded within 38 CFR 3.317(d), that potentially are associated with the infectious diseases listed in 38 CFR 3.317(c)(2). These health effects and diseases are listed alphabetically and are not categorized by the level of association stated in the National Academy of Sciences report. If a Veteran who has or had an infectious disease identified in column A also has a condition identified in column B as potentially related to that infectious disease, VA must determine, based on the evidence in each case, whether the column B condition was caused by the infectious disease for purposes of paying disability compensation. This does not preclude a finding that other manifestations of disability or secondary conditions were caused by an infectious disease. See 38 CFR 3.317(d) - Long-term health effects potentially associated with infectious diseases.
-
If a veteran presumed service connected for one of the diseases listed in 38 CFR 3.317(c)(2) is diagnosed with one of the diseases listed in column “B” in the table embedded within 38 CFR 3.317(d) within the time period specified for the disease in the same table, if a time period is specified or, otherwise, at any time, VA will request a medical opinion as to whether it is at least as likely as not that the condition was caused by the veteran having had the associated disease in column “A” in that same table. See 38 CFR 3.317(d) - Long-term health effects potentially associated with infectious diseases.
Notes
-
When evaluating any claim involving loss or loss of use of one or more creative organs, refer to 38 CFR 3.350 of this chapter to determine whether the Veteran may be entitled to special monthly compensation. Footnotes in the schedule indicate conditions which potentially establish entitlement to special monthly compensation; however, there are other conditions in this section which under certain circumstances also establish entitlement to special monthly compensation.