7351 - Liver transplant
DBQ: Link to Index of DBQ/Exams by Disability for DC 7351
Acronym: LITRA
Definition
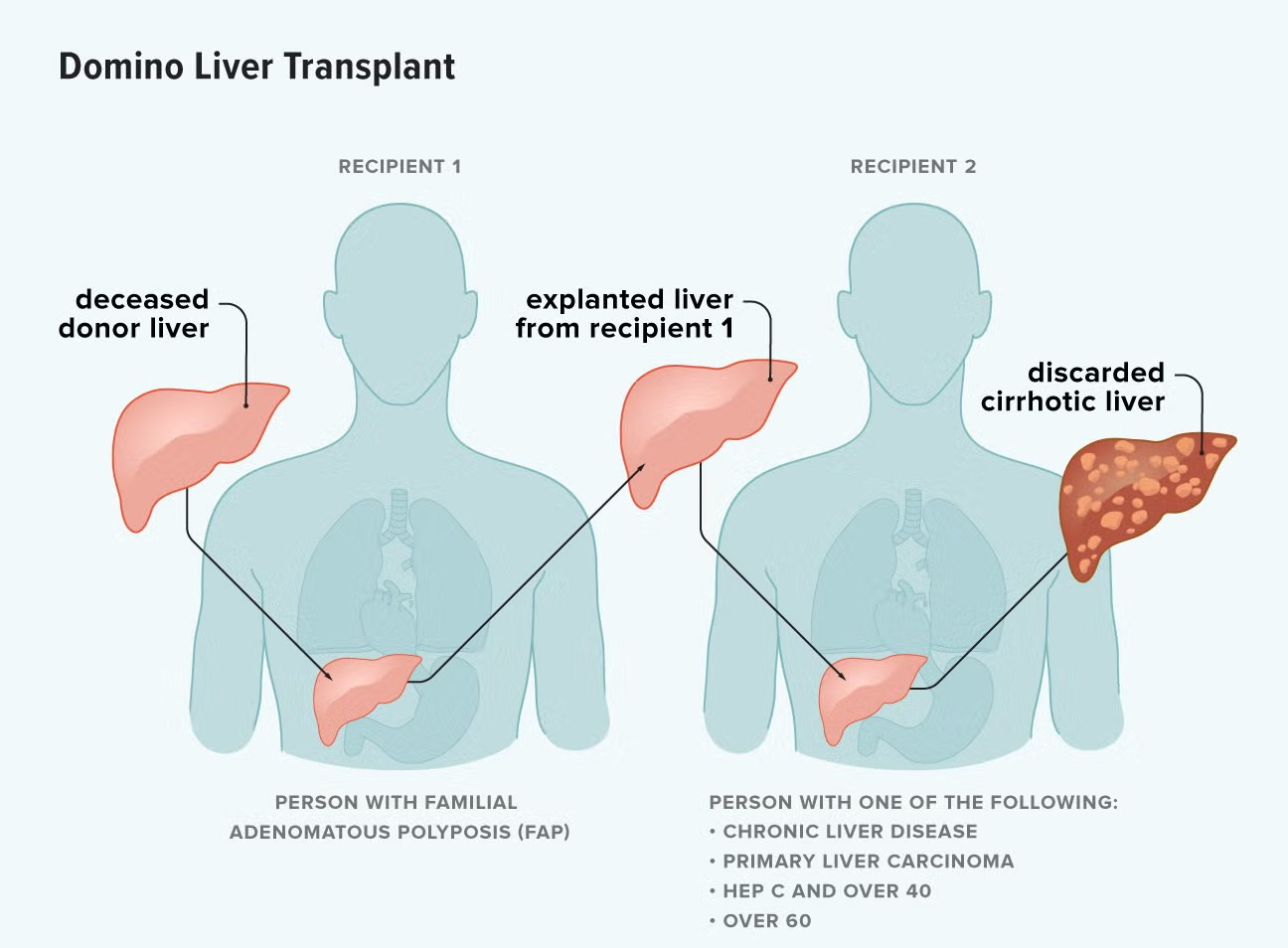
Transplantation of the liver is a process of transferring living tissues of the liver, or of the actual organ from one person to another to repair a defect. Liver transplantation is sometimes called hepatic transplantation.
{kind=link}
{kind=link}
{kind=link}
Etiology
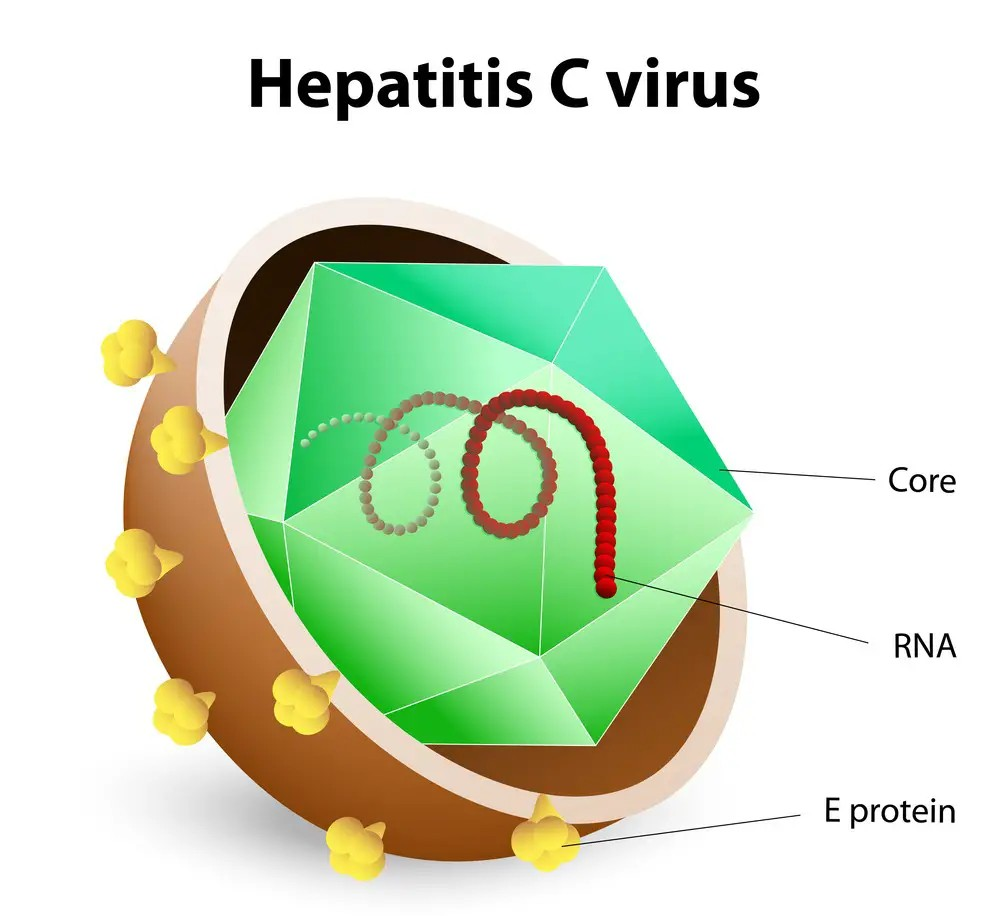
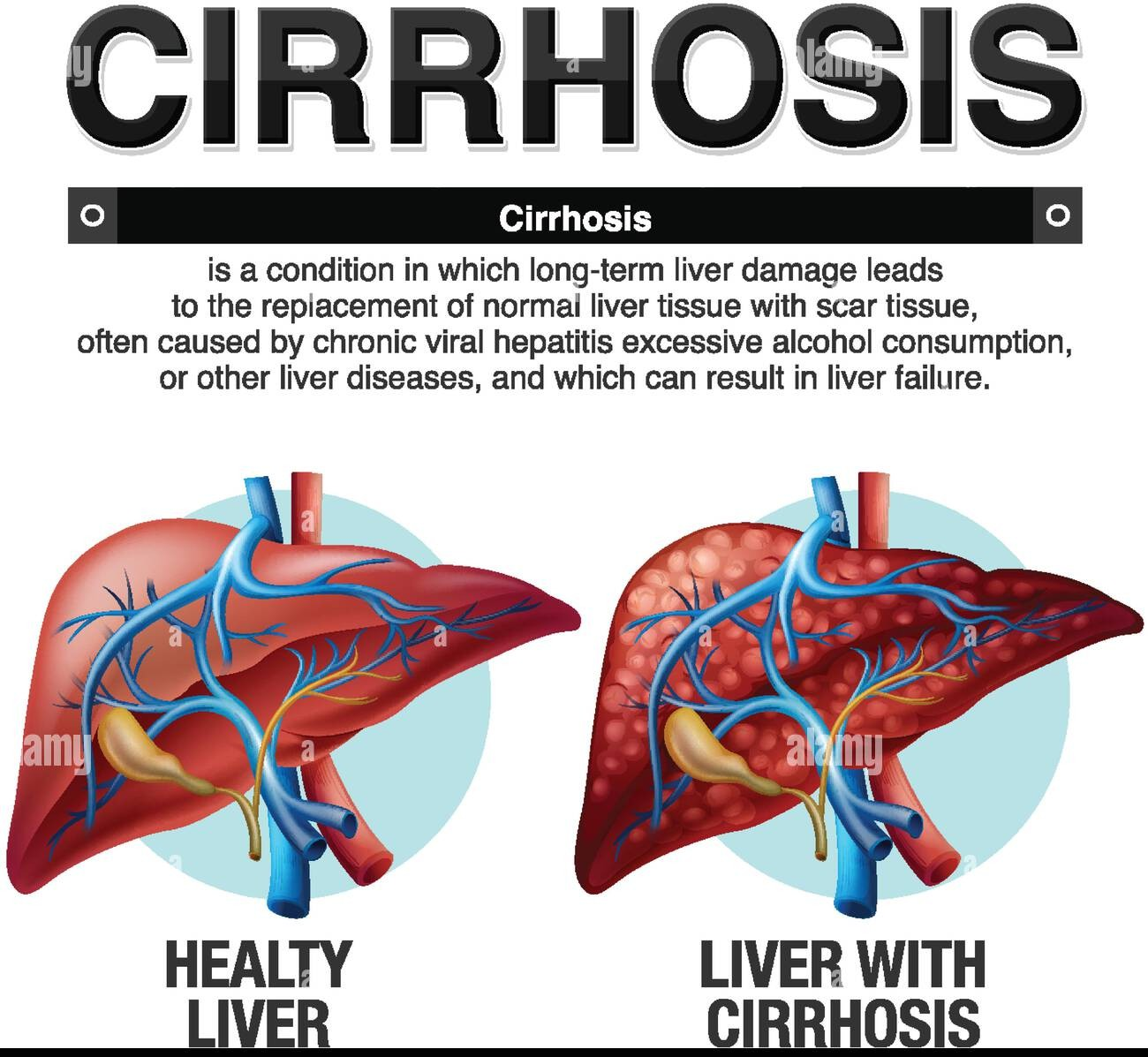
Liver transplantation is the treatment for patients with irreversible liver disease. Hepatitis C infection is now the leading cause for the procedure. Cirrhosis of the liver, resulting from hepatitis, is a major indication for the grafting procedure. End-stage chronic hepatitis and biliary cirrhosis, resulting in chronic liver failure, are the most frequent indications for the procedure. Other indications include: congenital biliary abnormalities; inborn errors of metabolism; hepatic malignancy confined to the liver; sclerosing cholangitis; and end-stage liver disease.
{kind=link}
{kind=link}
Signs & Symptoms
Manifestations related to irreversible and end-stage liver dysfunction serve as the basis for consideration of patients for transplantation. The exception is those at risk for non-hepatic life-threatening conditions and those unable to comply with the complex medical regimen. Signs and symptoms of end-stage liver disease include: hepatomegaly; ascites; jaundice; fatigue; fever; headache; abdominal pain; dyspepsia; anorexia; nausea; vomiting; and diarrhea or constipation.
{kind=link}
Tests
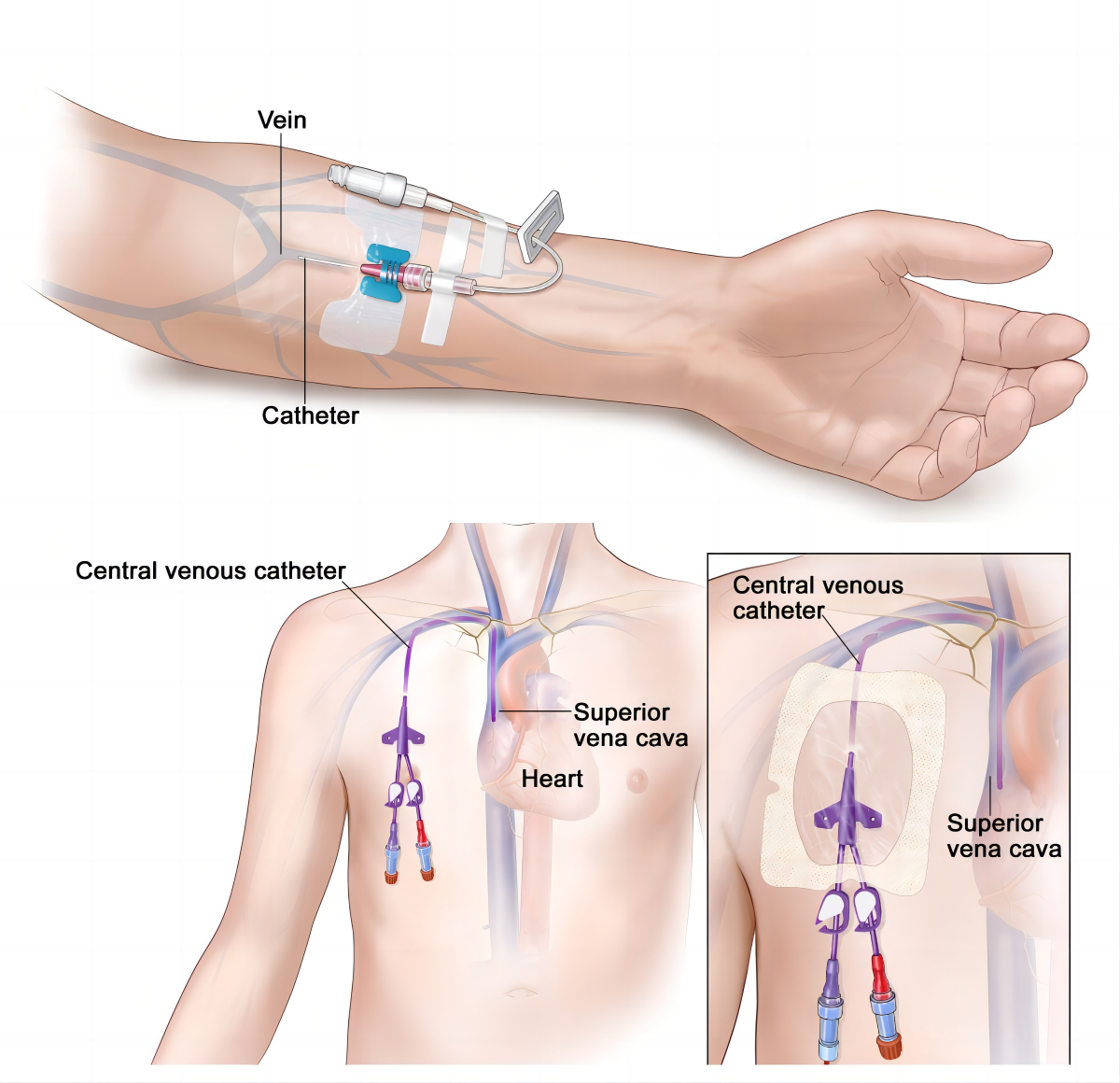
Prior to liver transplantation, normally scheduled preoperative measures are performed, e.g., physical examination, laboratory tests to identify infection, electrolyte studies, abdominal x-rays, electrocardiogram (EKG) and echocardiography. In addition to routine blood tests, other tests performed to confirm liver disease include: liver biopsy and liver scans; cholecystography; splenoportal venography; and intravenous (IV) and percutaneous transhepatic cholangiography.
{kind=link}
{kind=link}
{kind=link}
Treatment
Transplantation is the treatment for end-stage liver dysfunction. Prior to transplantation, patients require a great deal of preparation and support. There are a number of antirejection medications, classified as immunosuppressants, which are given postoperatively to allay rejection. However, cyclosporine is the most common drug used. Patients are advised to avoid contact with persons who have or may have contagious illnesses. The first 2 months are critical in terms of monitoring for infection. Emotional support and teaching of the patient and family are essential. After liver transplantation, patients are required to remain on immunosuppressant therapy for the rest of their lives.
Residuals
Postoperative compliance by the patient with all medications is extremely critical. Noncompliance can trigger rejection, even if a liver has been functioning well for years. The patient will require continuous reassurance and emotional support throughout the prolonged recovery period. The patient and family may seek psychological counseling to cope with the effects of the patient's long and difficult recovery. There may be side effects of the immunosuppressive drug therapy, such as infection, fluid retention, hypertension, psychoses, seizures, acne, glaucoma, diabetes and cancer. Patients who have liver disease secondary to viral hepatitis may experience reinfection of the graft with hepatitis. The patient must be monitored for opportunistic infections that can lead to rejection. Regular follow-up examinations are required.
Special Considerations
-
May be entitled to special monthly compensation where the Veteran has a single service-connected disability rated as 100% with additional service-connected disability or disabilities independently ratable at 60% or more, which are separate and distinct from the 100% service-connected disability and involves different anatomical segments or bodily systems. See 38 CFR 3.350(i)(1) – Special Monthly Compensation (SMC).
Notes
-
A rating of 100 percent shall be assigned as of the date of hospital admission for transplant surgery and shall continue. One year following discharge, the appropriate disability rating shall be determined by mandatory VA examination. Any change in evaluation based upon that or any subsequent examination shall be subject to the provisions of 38 CFR 3.105(e) of this chapter.