7347 - Pancreatitis, chronic
DBQ: Link to Index of DBQ/Exams by Disability for DC 7347
Acronym: PACRI
Definition
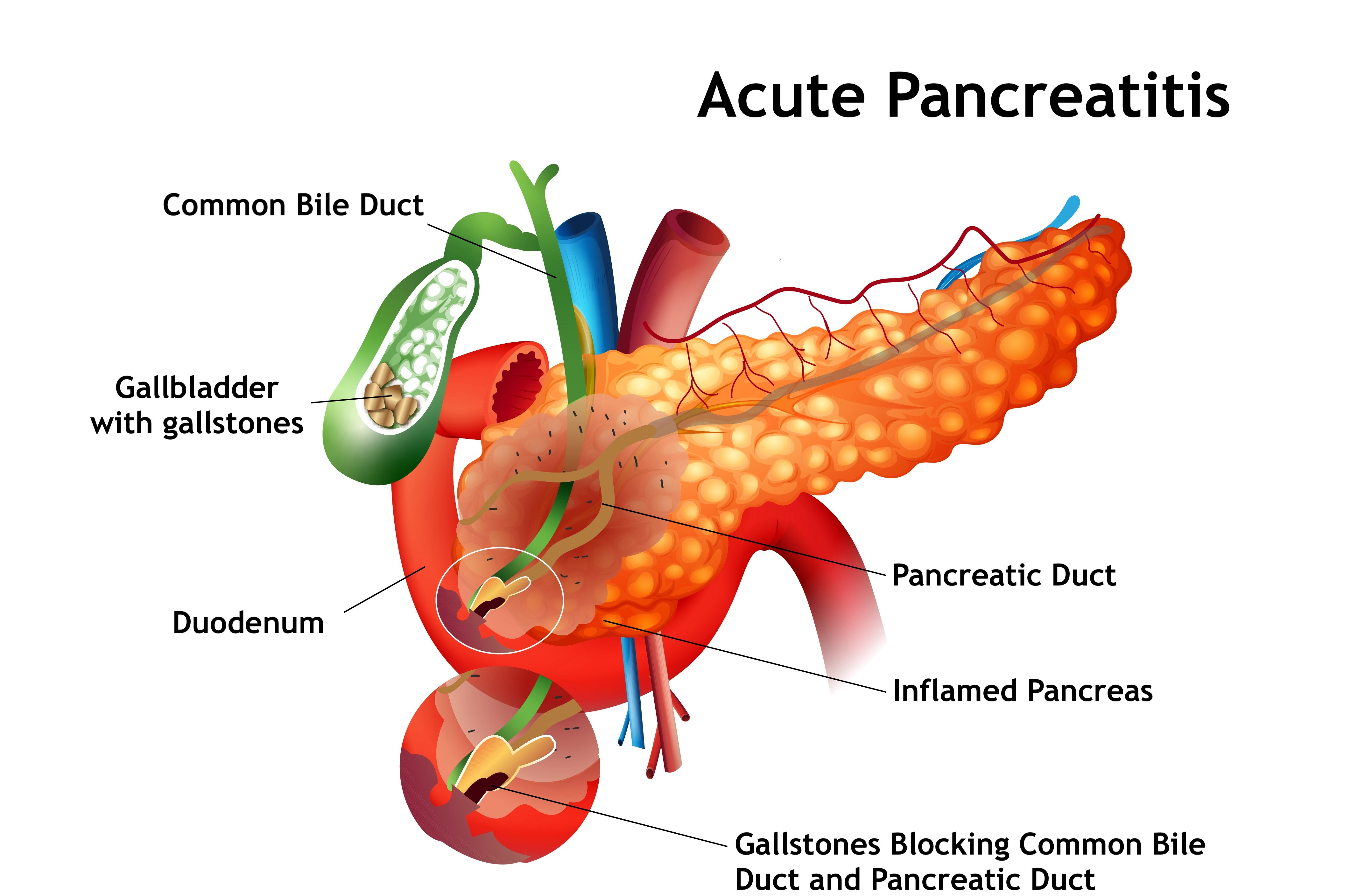
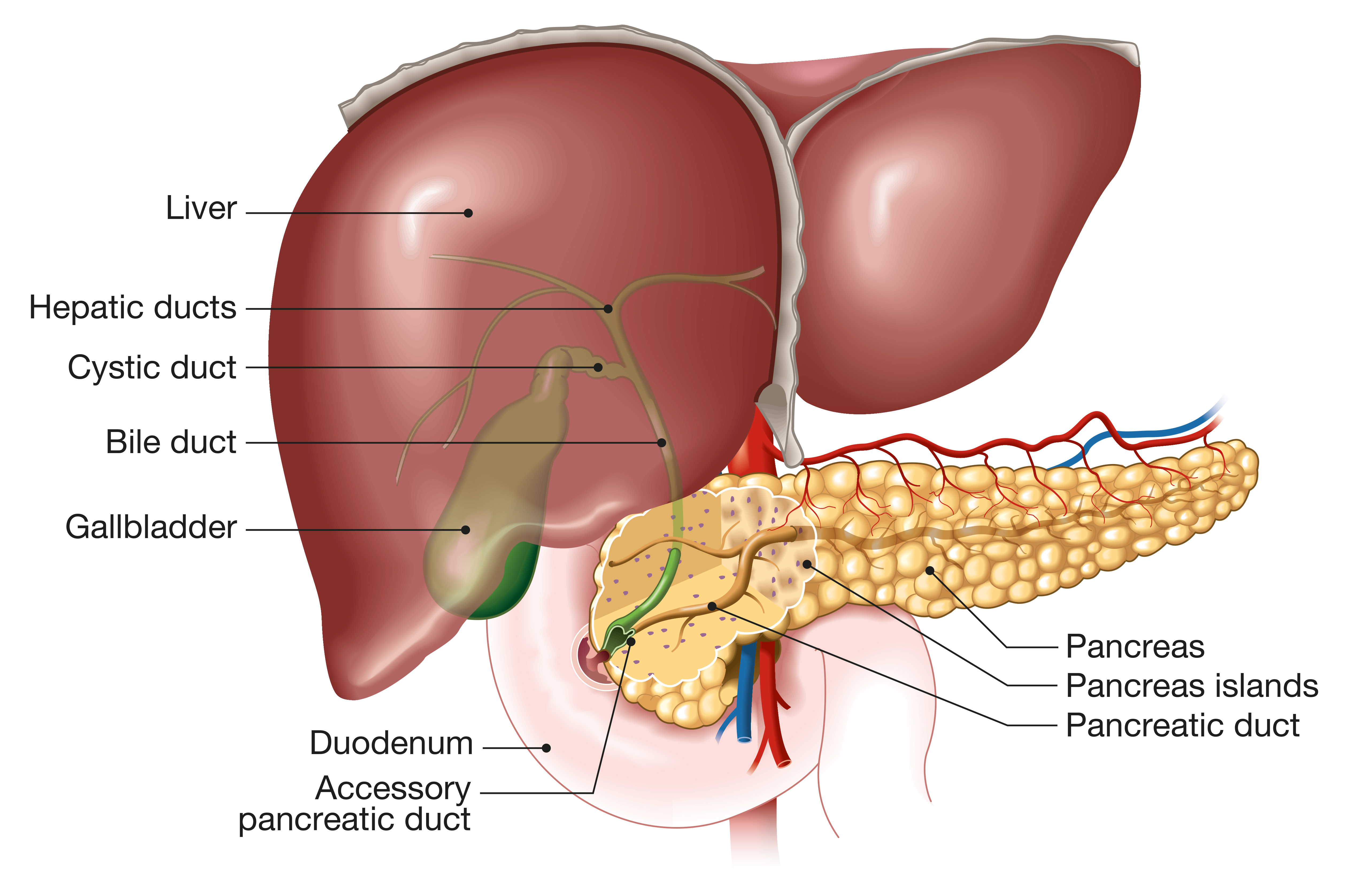
Pancreatitis refers to the inflammation of the pancreas. The pancreas is a gland located behind the stomach with a part that secretes a substance to assist with the digestion of foods in the small intestine, and another part that secretes substances directly into the bloodstream. This inflammation may be acute or chronic. Inflammation is a response in a body part that is related to a wide variety of agents resulting in abnormal changes in the functioning of the body part. In this case, the inflammation of the pancreas may be acute or chronic.
{kind=link}
{kind=link}
Etiology
Etiologic factors related to the acute and chronic forms of pancreatitis are as follows:
-
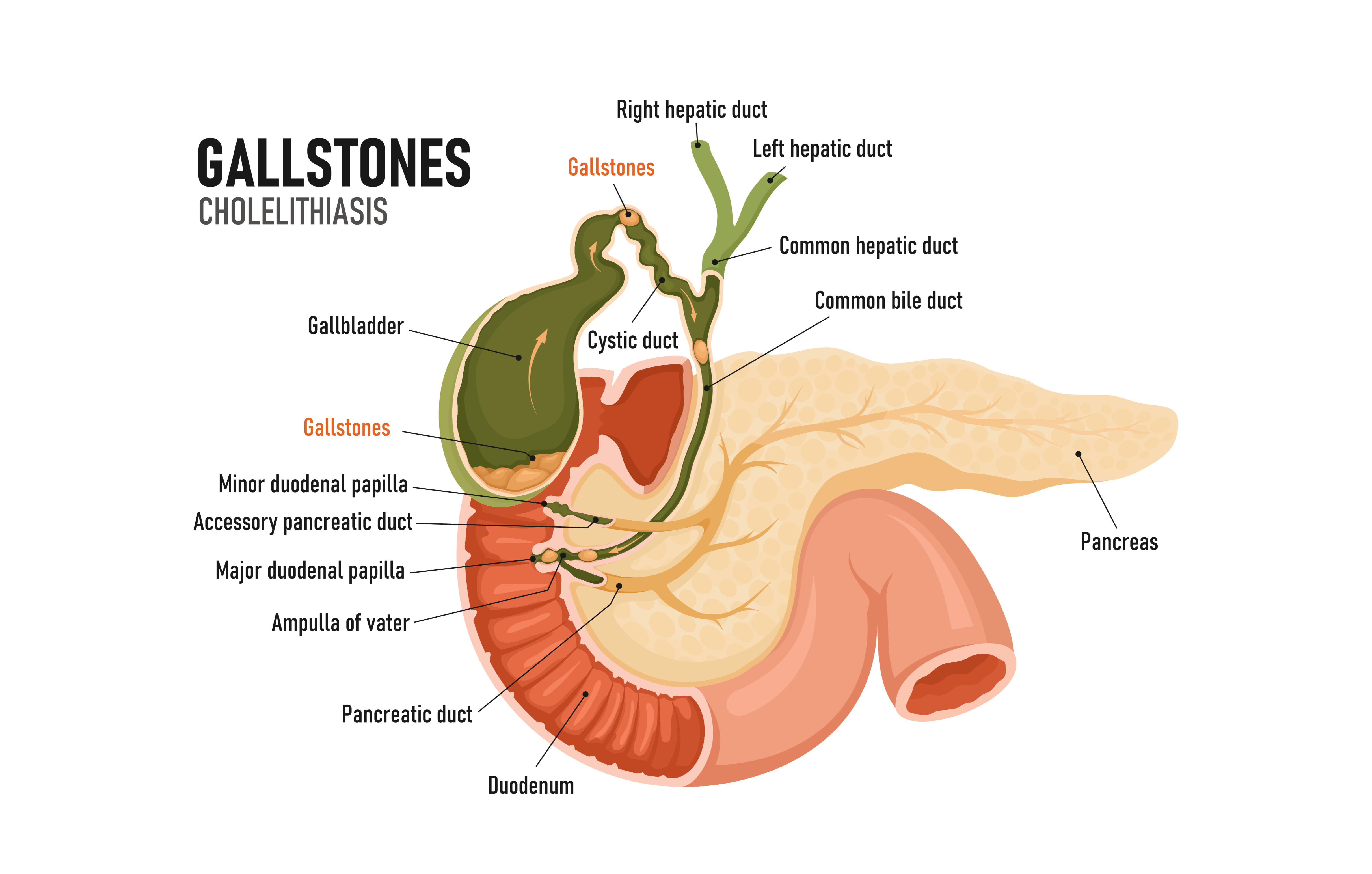
Acute - May be caused by overuse of alcohol; biliary tract disease (gallstones); certain drugs; increased triglyceride or calcium levels in the blood; and viral or bacterial infections.
-
Chronic- May involve a history of alcohol abuse, and obstruction of the common bile duct by stones, stenosis, or cancer. The exact cause may be unknown.
{kind=link}
Signs & Symptoms
Manifestation of the acute and chronic forms of pancreatitis are as follows:
-
Acute - Twelve to twenty-four hours after a bout of drinking alcohol or eating a heavy meal, an intense pain of long duration that radiates to the back and chest develops. Other signs and symptoms include: cold, clammy skin; fever; abdominal distention and tenderness; and nausea and vomiting.
-
Chronic - Symptoms develop slowly over years in episodes of acute attacks. Signs and symptoms include: pain that is long-lasting and radiates to the back and chest; stools that are bulky and foul smelling; weight loss; nausea and vomiting; clammy cold skin and fever; and the onset of diabetes mellitus.
Tests
Diagnostic measures may involve serum amylase and lipase concentration tests which show marked increases, and then the levels return to normal usually within seven days. In addition, abdominal x-rays may show stones in the pancreatic ducts or in the gallbladder, and a chest film may reveal left-sided pleural effusion. Other measures include: ultrasound; computed tomography (CT) scan; and magnetic resonance imaging (MRI).
{kind=link}
{kind=link}
{kind=link}
Treatment
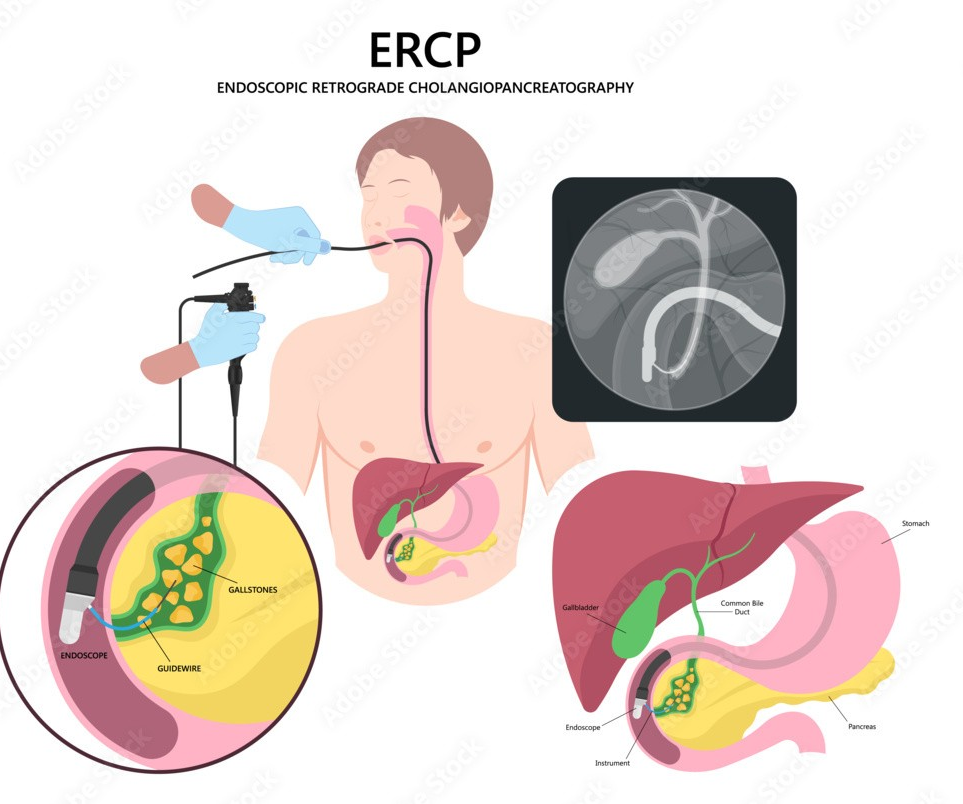
In acute, mild edematous pancreatitis, the patient is required to fast until the acute inflammation symptoms subside. Intravenous fluids are used for hydration if vomiting and an ileus are present. A tube is then passed into the stomach to keep it empty. If the pancreatitis is caused by an obstructed gallbladder or pancreas, surgery may be necessary after the inflammation has subsided. A stone in the duct of the pancreas or at the common entrance to the small intestine is removed by an endoscope in a procedure called endoscopic retrograde cholangiopancreatography (ERCP). Severe acute pancreatitis may be life-threatening, and require hospitalization in an intensive care unit. This patient may not be fed for more than 4 weeks. During this period, fluid replacement is crucial, oxygen therapy is initiated, and blood levels of glucose, calcium and magnesium are closely monitored. Dialysis may become necessary for renal failure.
{kind=link}
The treatment of chronic pancreatitis is focused on two problems: pain and malabsorption. Use of a pain reliever carries the threat of addiction since the pain is not easily relieved. Pancreatic replacement therapy is used for the malabsorption syndrome, which requires many pills a day. In diabetes mellitus associated with chronic pancreatitis, most patients have blood glucose levels of 200 to 250 mg/dL. This is acceptable and not treated because the greater risk is hypoglycemia. A relapse of chronic pancreatisis is treated similarly to the treatment of the acute condition.
Residuals
Acute pancreatitis may be fatal during the first weeks due to toxins and circulating enzymes that result in shock, and respiratory, renal or heart failure. There is an increased risk for pancreatic cancer in patients with chronic pancreatitis.
Special Considerations
-
May be entitled to special monthly compensation where the Veteran has a single service-connected disability rated as 100% with additional service-connected disability or disabilities independently ratable at 60% or more, which are separate and distinct from the 100% service-connected disability and involves different anatomical segments or bodily systems. See 38 CFR 3.350(i)(1) – Special Monthly Compensation (SMC).
-
May require a line of duty determination under 38 CFR 3.301(d) [Line of duty; abuse of alcohol or drugs].
Notes
-
Abdominal pain in this condition must be confirmed as resulting from pancreatitis by appropriate laboratory and clinical studies.
-
Following total or partial pancreatectomy, rate under above, symptoms, minimum rating 30 percent.
-
Ratings under diagnostic codes 7301 to 7329, inclusive, 7331, 7342, and 7345 to 7348 inclusive will not be combined with each other. A single evaluation will be assigned under the diagnostic code which reflects the predominant disability picture, with elevation to the next higher evaluation where the severity of the overall disability warrants such elevation. [38 CR 4.114]
-
There are diseases of the digestive system, particularly within the abdomen, which, while differing in the site of pathology, produce a common disability picture characterized in the main by varying degrees of abdominal distress or pain, anemia and disturbances in nutrition. Consequently, certain coexisting diseases in this area, as indicated in the instruction under the title “Diseases of the Digestive System,” do not lend themselves to distinct and separate disability evaluations without violating the fundamental principle relating to pyramiding as outlined in 38 CR 4.14. [38 CFR 4.113]