7345 - Chronic liver disease without cirrhosis
DBQ: Link to Index of DBQ/Exams by Disability for DC 7345
Definition
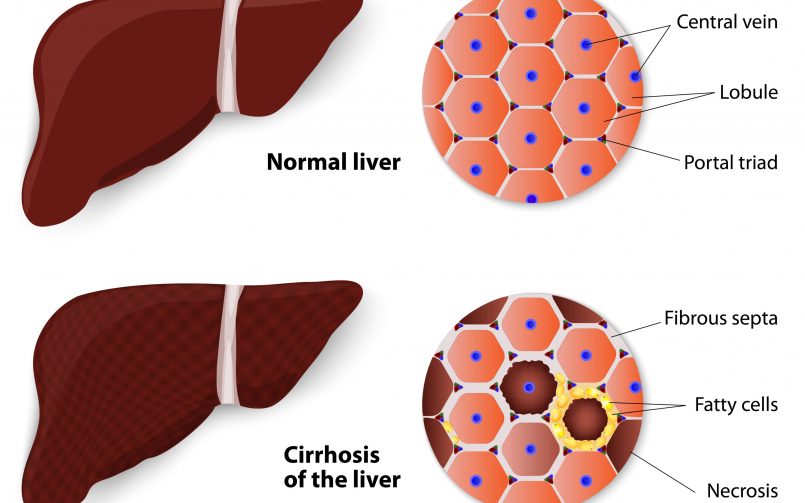
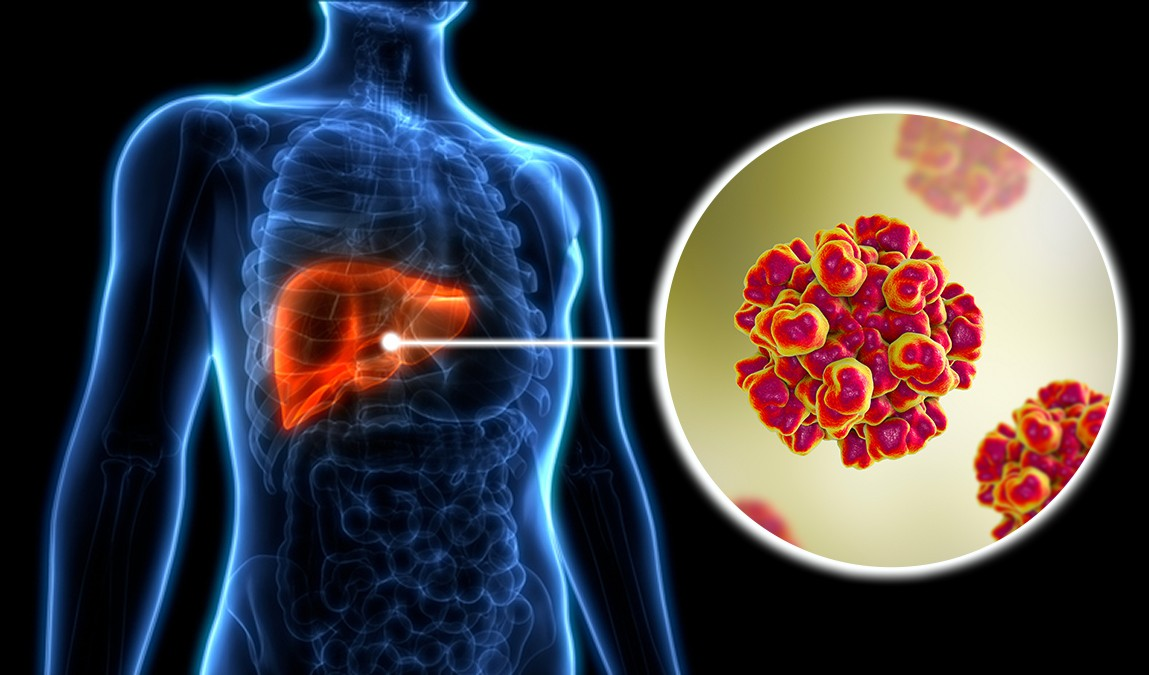
Chronic liver disease is marked by the gradual destruction of liver tissue over time. Infectious hepatitis was formerly the term used to describe Hepatitis A (HAV). However, at least six forms of infectious hepatitis presently exist in humans. The term infectious refers to a condition caused by the invasion of microorganisms in tissues which results in infection. In infectious hepatitis, an inflammation of the liver is present. The inflammation represents a reaction to microorganisms in the liver causing functional disturbances in the organ. The liver is located underneath the diaphragm and is the organ where many metabolic functions occur.
{kind=link}
Etiology
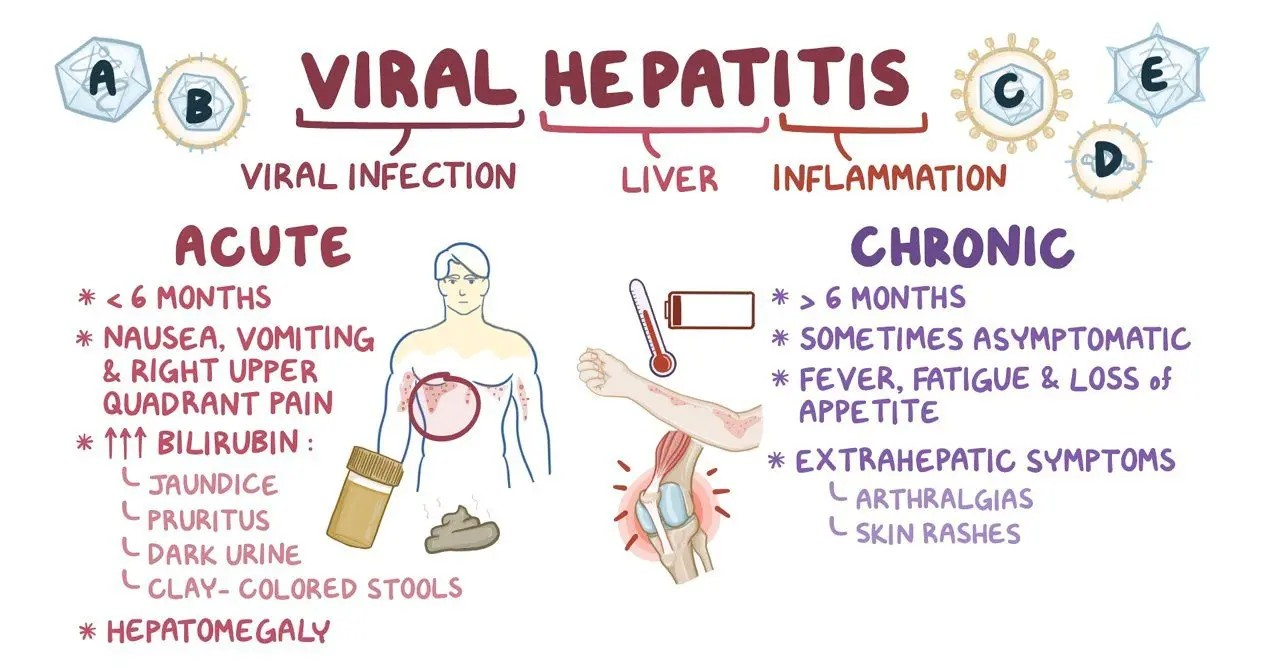
Viruses identified as being responsible for acute viral hepatitis are: Hepatitis A virus (HAV); Hepatitis B virus (HBV); Hepatitis D virus (HDV); Hepatitis E virus (HEV); and Hepatitis G virus (HGV). The importance of human disease is not yet well-defined for Hepatitis F virus (HFV). This form is thought to be transmitted by the anal-oral route. Characteristics related to the six specific viruses are as follows:
-
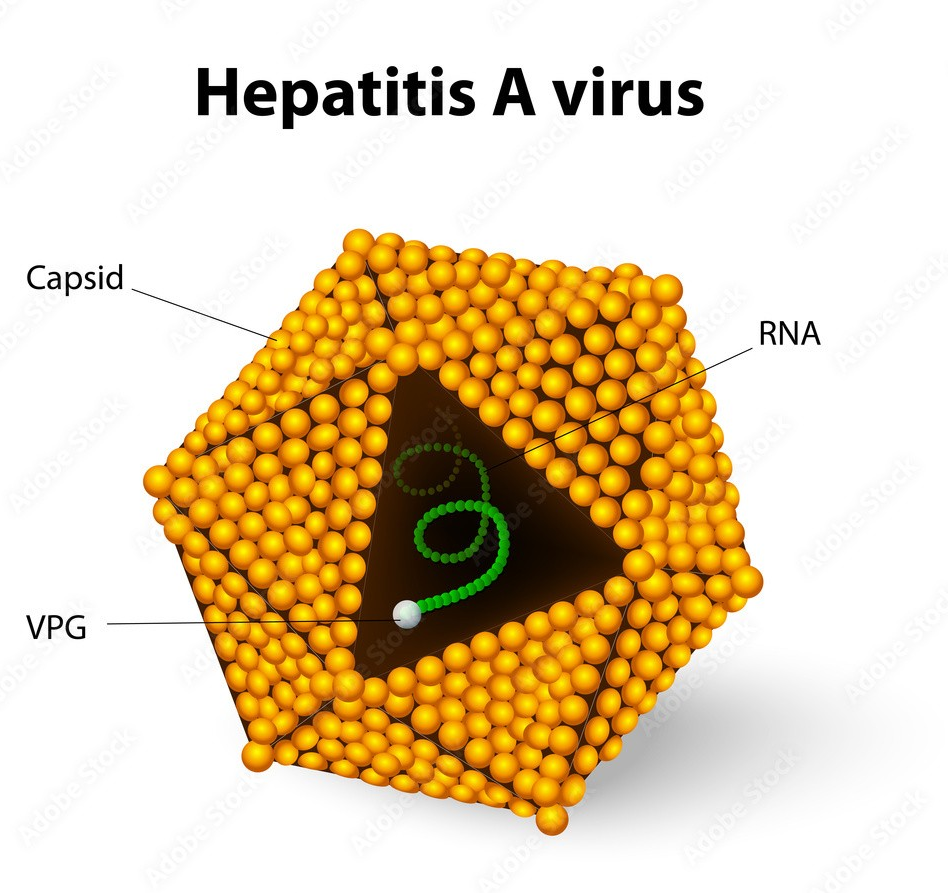
Hepatitis A virus - The organism is found in blood and stool and in the liver during the acute stage of the infection. The infection is contracted mainly through contaminated food or water. Epidemics occur in underdeveloped countries. There is no known carrier state.
-
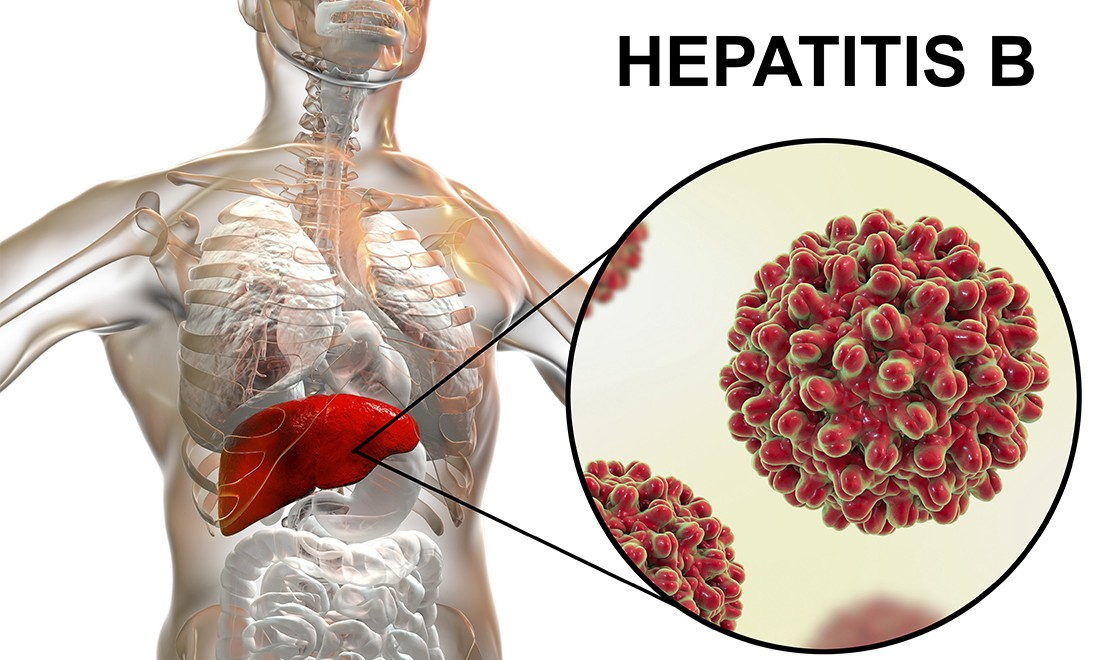
Hepatitis B virus - The major method of transmission is by blood or blood products, the sharing of needles by drug abusers, and articles contaminated with blood, e.g., razors, toothbrushes and dentist's appliances. Carriers of HBV are responsible for spread of the disease, and sexual transmission is prevalent.
-
Hepatitis D virus - The major means of transmission is by needle. It appears as a co-infection with HBV. In several countries there are endemic areas. Most infections in the Western world are related to intravenous (IV) drug abuse; however, sexual transmission can occur.
-
Hepatitis E virus - The major transmission is thought to be by water. It is responsible for epidemics of acute hepatitis. Outbreaks are found in developing countries.
-
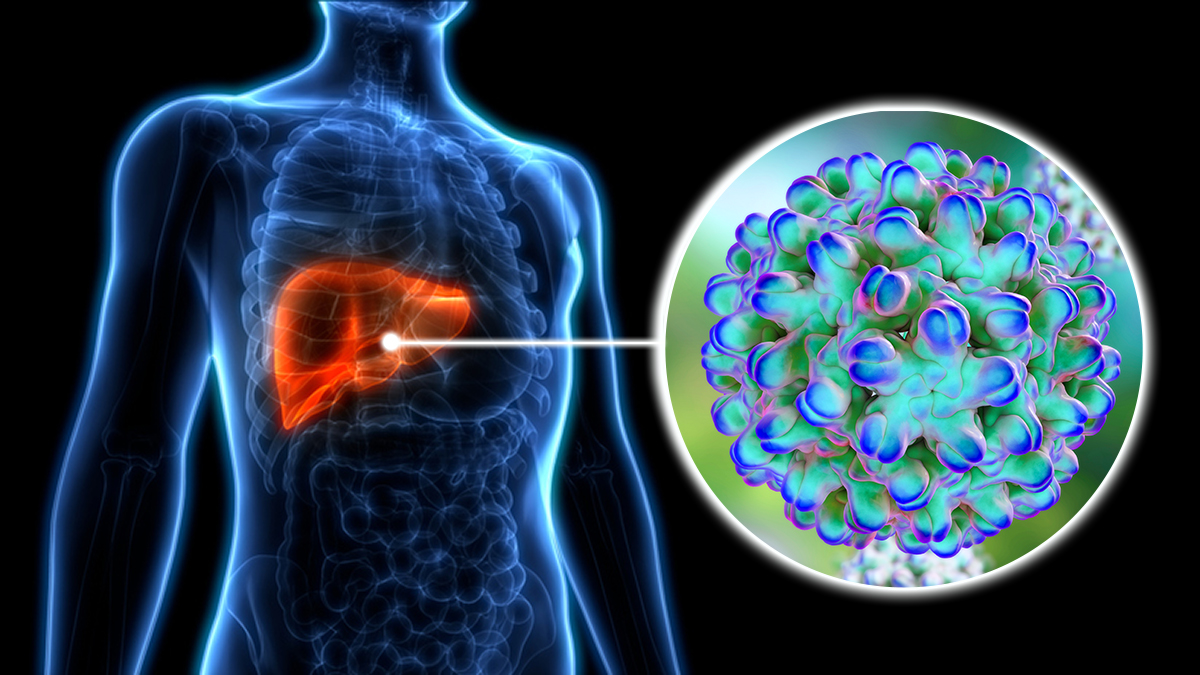
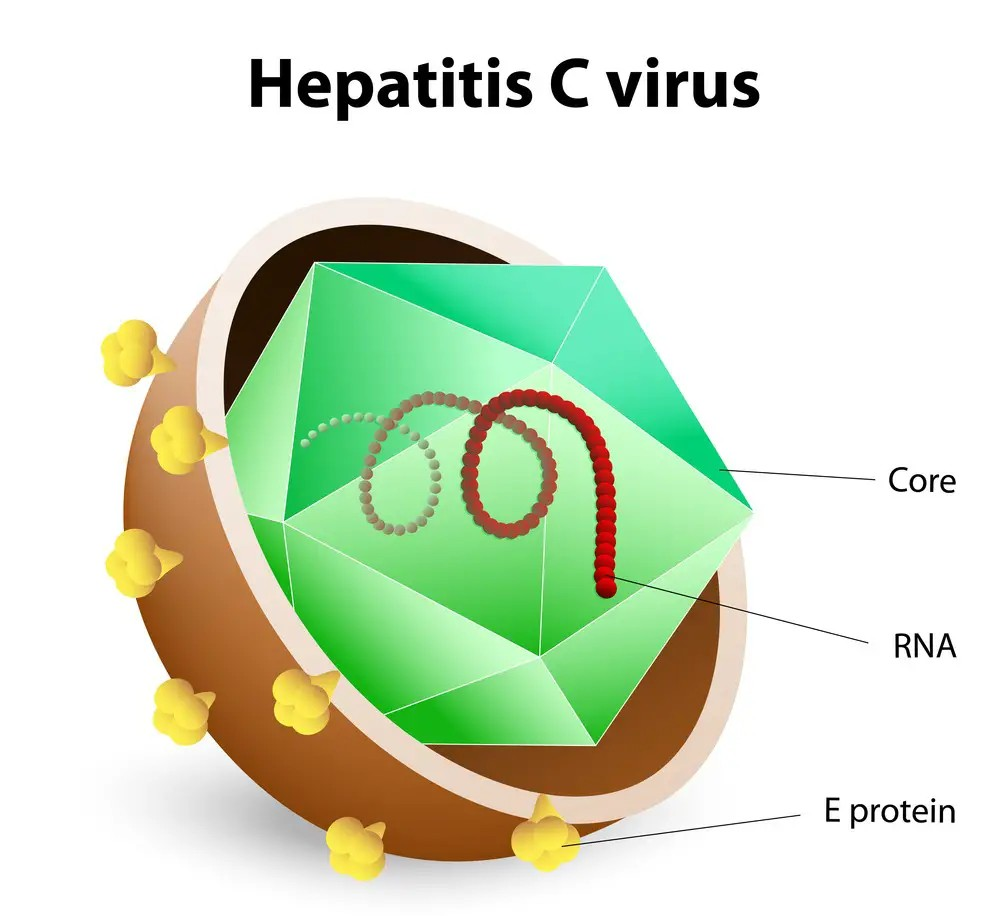
Hepatitis G virus - This form can be transmitted by blood, and may be related to chronic hepatitis. However, the major mode of transmission has not been established. The condition is often associated with HBV and HCV infections. IV drug use may be a factor in the incidence of the condition.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Signs & Symptoms
The stage of infection or disease and the age of the patient are factors that affect the signs and symptoms of most liver conditions. However, the manifestations for all of the causative viruses are similar. The primary clinical signs are hepatomegaly and jaundice. The onset is either abrupt or gradual. In the early course of the disease, the patient demonstrates signs and symptoms including: fatigue; low-grade fever; headache; muscle and joint pain; loss of appetite; disorders of taste and smell; nausea and vomiting; dark urine; and clay-colored stools. The liver is enlarged and fever is present during the preicteric phase. When the icteric phase begins, jaundice develops as early symptoms worsen; the urine is darker and the stools more clay-colored. The skin and sclera are jaundiced; pruritus may present; and the liver remains enlarged and tender. During the next phase (convalescent phase) which lasts 2 to 12 weeks, pain, fatigue, and indigestion may continue until recovery is achieved. During the recovery period, signs and symptoms decrease.
Tests
A significant factor in the diagnosis of acute viral hepatitis is observations of the reactions of blood serum. General serologic studies may include determinations including: hyperglobulinemia; prolonged prothrombin time; hypoglycemia; leukocytosis; hemoglobin and hematocrit; and the presence of bilirubin in the urine. Confirmation of the phases or stages of Hepatitis A, B, D, and E viruses is determined by specific etiologic diagnostic tests. Blood tests are performed to detect the presence of antigens and antibodies related to the specific type of Hepatitis.
Treatment
Specific measures of treatment may not be needed. Control of activity by bedrest, although routine in the past, is not considered to be necessary. Patient's activity is monitored by their response to activity. Those with severe damage, or the elderly, may require greater modification than others. Dietary modifications may include food intake that is low in fat, high in calories, nutritious in content and adequate in fluids. IV feeding may be necessary if oral intake is limited because of vomiting. Avoidance of alcohol intake is generally recommended. The use of corticosteroids is questionable. Some authorities suggest complete avoidance, while others limit the therapy to specific circumstances.
Emphasis is given to prevention of the condition because of the lack of specific treatment of acute viral hepatitis and the limited success of measures to suppress or destroy viruses in chronic viral hepatitis.
Despite the development of effective vaccines to prevent two forms of viral hepatitis, HAV and HBV, and the expectant progress in the development of vaccines for the other forms, the need for measures to prevent exposure to infectious material still exists. Public health measures and those related to hygiene depend on the following factors: the organism involved; the stage of the disease; the type of infectious material; the method of transmission; and the kind of exposure.
Standard immune globulin has been used to protect household contacts of patients and travelers to endemic areas against HAV and HBV. Hepatitis B immune globulin (HBIG) is given to persons with accidental sticks from needles, exposure to blood contaminated by the HBV virus, and sexual contacts of patients with HBV.
{kind=link}
{kind=link}
Residuals
Decisions made relative to return to work are dependent upon the patient's symptoms, the nature of the work, and the likelihood of transmission of the disease. In general, with hepatitis A, within about 2 to 3 weeks, the patient is unlikely to spread the infection. However, in terms of hepatitis B, personal contact is the basis for the spread of these conditions. Patient and family support may be required due to the duration of symptoms and the requirements needed for care of the patient.
After about 4 to 8 weeks, spontaneous resolution of hepatitis A is generally expected. The expectation for resolution is less favorable in hepatitis B, especially for the elderly. Chronic HBV infection occurs in about 5% to 10% of patients, which can lead to cancer. The highest level of chronicity is presented by HCV. Late cirrhosis may appear years after the initial condition, and cancer is a risk.
{kind=link}
Special Considerations
-
May be entitled to special monthly compensation where the Veteran has a single service-connected disability rated as 100% with additional service-connected disability or disabilities independently ratable at 60% or more, which are separate and distinct from the 100% service-connected disability and involves different anatomical segments or bodily systems. See 38 CFR 3.350(i)(1) – Total plus 60% – Special Monthly Compensation (SMC).
-
Fatty liver, also called hepatic steatosis, is not a disability for which SC can be granted. By itself it is simply considered an abnormal laboratory finding.
{kind=link}
Notes
-
Evaluate sequelae, such as cirrhosis or malignancy of the liver, under an appropriate diagnostic code, but do not use the same signs and symptoms as the basis for evaluation under DC 7354 and under a diagnostic code for sequelae. (See 38 CFR 4.14.).
-
For purposes of evaluating conditions under diagnostic code 7345, “incapacitating episode” means a period of acute signs and symptoms severe enough to require bed rest and treatment by a physician.
-
Hepatitis B infection must be confirmed by serologic testing in order to evaluate it under diagnostic code 7345.
-
Ratings under diagnostic codes 7301 to 7329, inclusive, 7331, 7342, and 7345 to 7348 inclusive will not be combined with each other. A single evaluation will be assigned under the diagnostic code which reflects the predominant disability picture, with elevation to the next higher evaluation where the severity of the overall disability warrants such elevation. [38 CR 4.114]
-
There are diseases of the digestive system, particularly within the abdomen, which, while differing in the site of pathology, produce a common disability picture characterized in the main by varying degrees of abdominal distress or pain, anemia and disturbances in nutrition. Consequently, certain coexisting diseases in this area, as indicated in the instruction under the title “Diseases of the Digestive System,” do not lend themselves to distinct and separate disability evaluations without violating the fundamental principle relating to pyramiding as outlined in 38 CFR 4.14. [38 CFR 4.113]
-
For purposes of evaluating conditions in 38 CFR 4.114, the term “substantial weight loss” means a loss of greater than 20 percent of the individual's baseline weight, sustained for three months or longer; and the term “minor weight loss” means a weight loss of 10 to 20 percent of the individual's baseline weight, sustained for three months or longer. The term “inability to gain weight” means that there has been substantial weight loss with inability to regain it despite appropriate therapy. “Baseline weight” means the average weight for the two-year-period preceding onset of the disease. [38 CFR 4.112]