7338 - Hernia, including femoral, inguinal, umbilical, ventral, incisional, and other (but not including hiatal)
DBQ: Link to Index of DBQ/Exams by Disability for DC 7338
Definition
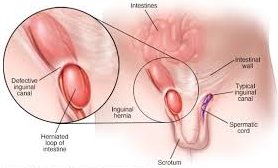
The inguinal area of the body is referred to as the groin. A hernia is a weak point in the abdominal wall where any part of an abdominal organ can protrude. With an inguinal hernia, the protrusion of the hernial sac containing the intestine is located at the inguinal ring.
{kind=link}
Etiology
Hernias result from weakened abdominal muscles. This weakness occurs as a result of injury, congenital malformation, aging, or conditions that increase the intra-abdominal pressure. Some of these conditions might be heavy lifting, straining, pregnancy or obesity.
Signs & Symptoms
Manifestations of the condition include a lump in the groin that appears when standing and disappears when lying down. In addition, pain occurs with lifting, especially if a person is bending at the same time. In an incarcerated hernia, the segment of intestine is trapped and cannot be pushed back up into the abdomen. A strangulated hernia occurs when the intestinal segment is trapped and the blood supply is cut off. The hernia may penetrate the scrotum in men. Symptoms of sharp pain, nausea and vomiting accompany strangulation.
Tests
A bulge near the pubic bone (right or left) can be felt on physical examination. When the bulge persists, and nausea and vomiting are present, the hernia may be incarcerated or strangulated. If a bowel obstruction is suspected, an abdominal x-ray and a white blood cell (WBC) count may be done prior to surgery.
Treatment
Surgery is the usual and preferred treatment for hernias. A strangulated hernia needs emergency surgery before the bowel becomes gangrenous. A corset or truss to keep the abdominal contents from protruding may be helpful while waiting for surgery, or for some elderly persons who cannot tolerate surgery.
Residuals
Normal activities may usually be resumed 4 to 6 weeks after surgery.
Special Considerations
-
Do not assume the preexistence of a hernia except on the basis of factual evidence. Thus initial manifestation of hernial protrusion in service is generally a sufficient basis for service connection, as is (by aggravation) recurrence during service of a hernia previously operated on or repaired. However, operation for repair of preexisting inguinal hernia is not, in itself, evidence of aggravation (it has to be absolutely clear in the records that the hernia existed prior to service, no symptoms were present and the surgery was elective).
Notes
-
With two compensable inguinal hernias, evaluate the more severely disabling hernia first, and then add 10% to that rating to account for the second compensable hernia. Do not add 10% to that rating if the more severely disabling hernia is rated at 100%.