7305 - Ulcer, duodenal
Removed from the rating schedule effective May 19, 2024
DBQ: Link to Index of DBQ/Exams by Disability for DC 7305
Definition
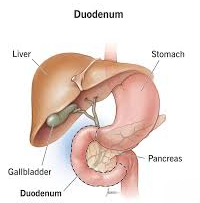
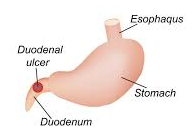
The duodenum is at the beginning of the small intestine situated between the pylorus and jejunum. In this case, the ulcer has eroded the mucosa, which penetrates the muscle layer, and is located in the first few centimeters of the structure. Duodenal ulcers account for more than half of peptic ulcer conditions.
{kind=link}
{kind=link}
Etiology
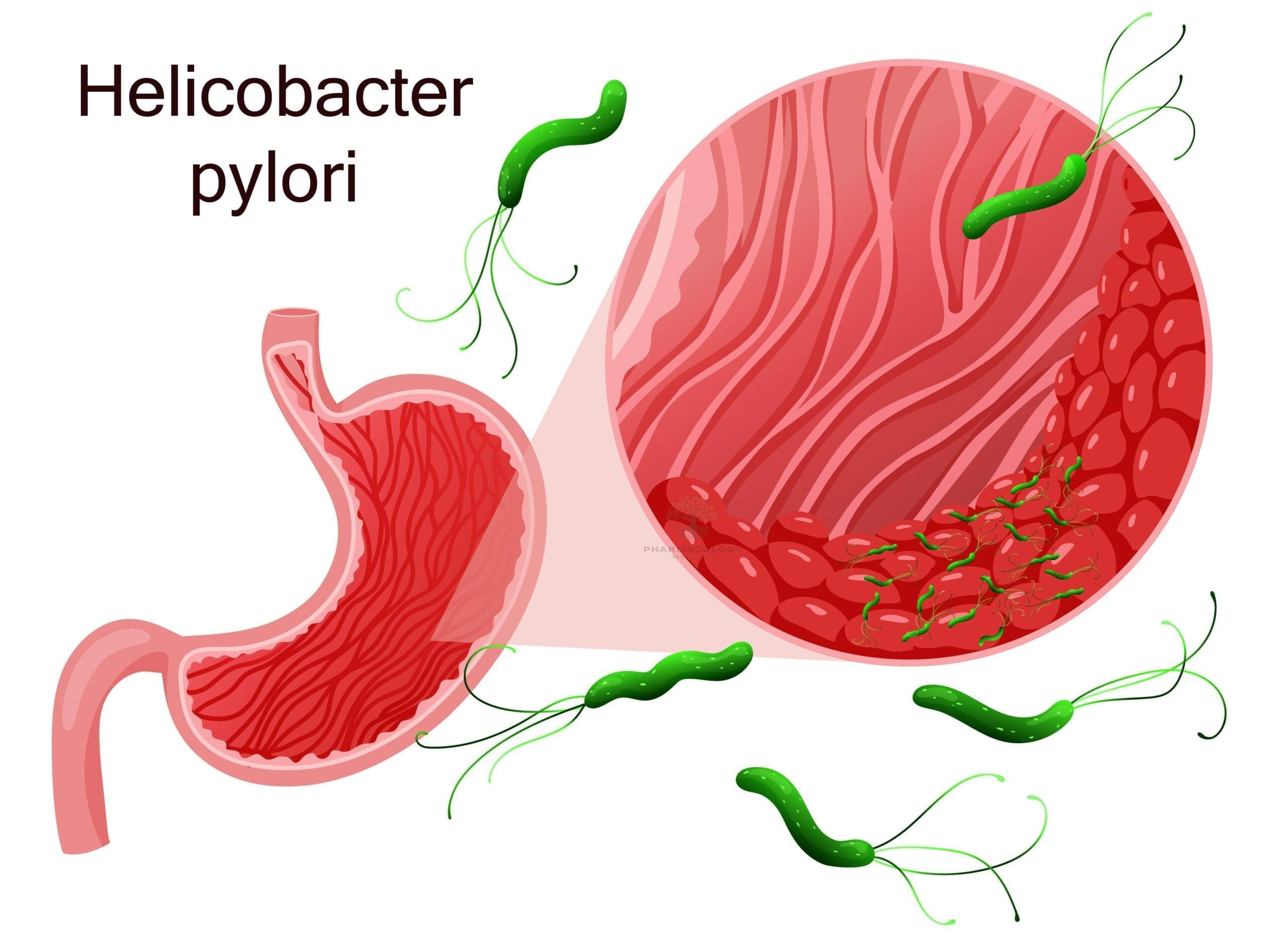
Heliobacter (H) pylori is a major factor in the development of ulcers. The bacterium disrupts the mucosal surface making it more likely to erode in the presence of acid. The use of nonsteroidal anti-inflammatory drugs (NSAID) and aspirin are also associated with ulcer formation.
{kind=link}
{kind=link}
Signs & Symptoms
Pain in duodenal ulcers usually follows a consistent pattern; absence upon awakening, appearance in midmorning, relief of pain by food, then recurrence of pain 2 to 3 hours after a meal. When a patient reports being awakened frequently with pain at night, the condition is most probably a duodenal ulcer. Belching, bloating and epigastric pain symptoms occur in over 50% of patients.
Tests
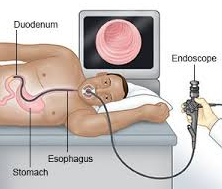
Endoscopy is recognized as an important diagnostic tool in duodenal ulcer. However, double contrast barium x-ray is utilized as an alternative method, and may be more helpful in detecting some duodenal ulcers.
{kind=link}
{kind=link}
Treatment
The main focus of treatment has shifted from neutralizing gastric acidity to eliminating H. pylori. Treatment with antibiotics is considered even if the patient is asymptomatic. Therapy consists of using more than one drug to reduce drug resistance. Histamine blocking drugs effectively suppress gastric acid and are used to reduce secretions. Proton pump inhibitors are long acting and can completely inhibit secretion of acid. Antacids must be taken 5 to 7 times a day to provide symptomatic relief. Special diets do not heal ulcers, and milk, which was formerly a part of treatment, has been found to increase acid secretion. Foods that cause distress should be eliminated, as well as the intake of alcohol. Smoking is inadvisable because it impairs ulcer healing. The new drug regimen has decreased the number of people needing surgery. However, poor response to medical management and complications of perforation, hemorrhage or obstruction would require surgical intervention.
Residuals
There is a relapse rate of over 60%. The reason for the relapse usually indicates that H. pylori were not eradicated. Thirty percent of patients who have surgery have significant problems with weight loss, poor digestion, anemia, a dumping syndrome, vomiting bile, recurrence of ulcer, bezoar formation, and diarrhea. Duodenal ulcers have a low incidence of malignancy.
Special Considerations
-
Anemia of chronic disease due to any GI disease should be rated together with the basic disease. If the anemia is pernicious and associated with neurological manifestations, it should be rated under code 37. Each manifestation, e.g., neuropathy and/or other neurologic involvement, should be rated separately.
-
This disease shall be granted service connection although not otherwise established as incurred in or aggravated by service if manifested to a compensable degree within the applicable time limits under 38 CFR 3.307 following service in a period of war or following peacetime service on or after January 1, 1947, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied [ 38 CFR 3.309 . [Disease subject to presumptive service connection], 38 CFR 3.309(a) [chronic disease].
-
If the Veteran is a former prisoner of war and was interned or detained for not less than 30 days, the following diseases shall be service connected if manifest to a degree of 10 percent or more at any time after discharge or release from active military, naval, air or space service even though there is no record of such disease during service, provided the rebuttable presumption provisions of38 CFR 3.307 are also satisfied. [38 CFR 3.309(c)(2)]
Notes
-
Ratings under diagnostic codes 7301 to 7329, inclusive, 7331, 7342, and 7345 to 7348 inclusive will not be combined with each other. A single evaluation will be assigned under the diagnostic code which reflects the predominant disability picture, with elevation to the next higher evaluation where the severity of the overall disability warrants such elevation. [38 CR 4.114]
-
There are diseases of the digestive system, particularly within the abdomen, which, while differing in the site of pathology, produce a common disability picture characterized in the main by varying degrees of abdominal distress or pain, anemia and disturbances in nutrition. Consequently, certain coexisting diseases in this area, as indicated in the instruction under the title “Diseases of the Digestive System,” do not lend themselves to distinct and separate disability evaluations without violating the fundamental principle relating to pyramiding as outlined in 38 CR 4.114. [38 CFR 4.113]
-
Experience has shown that the term “peptic ulcer” is not sufficiently specific for rating purposes. Manifest differences in ulcers of the stomach or duodenum in comparison with those at an anastomotic stoma are sufficiently recognized as to warrant two separate graduated descriptions. In evaluating the ulcer, care should be taken that the findings adequately identify the particular location. [38 CFR 4.110]