9900 - Maxilla or mandible, chronic osteomyelitis, osteonecrosis or osteoradionecrosis of
DBQ: Link to Index of DBQ/Exams by Disability for DC 9900
Definition
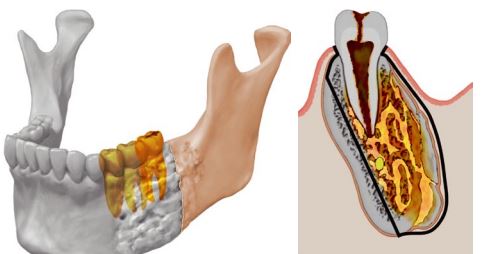
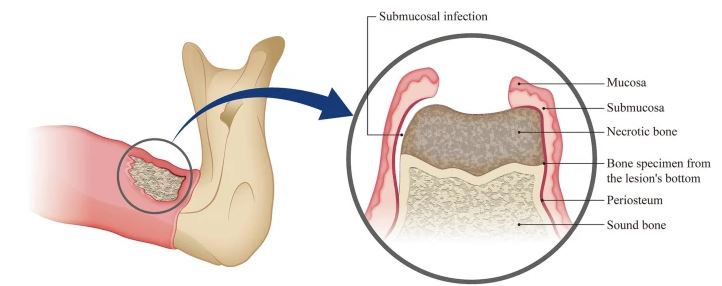
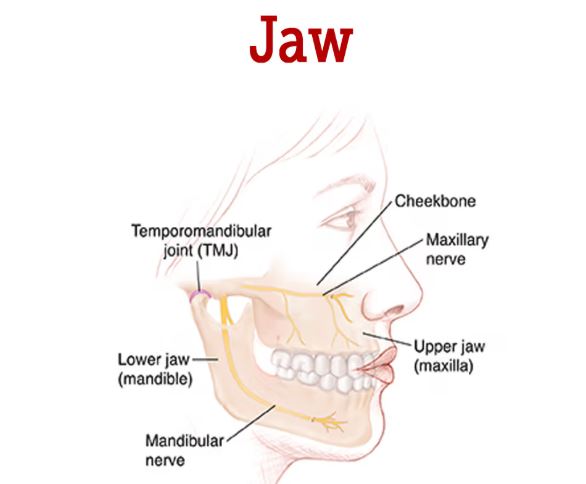
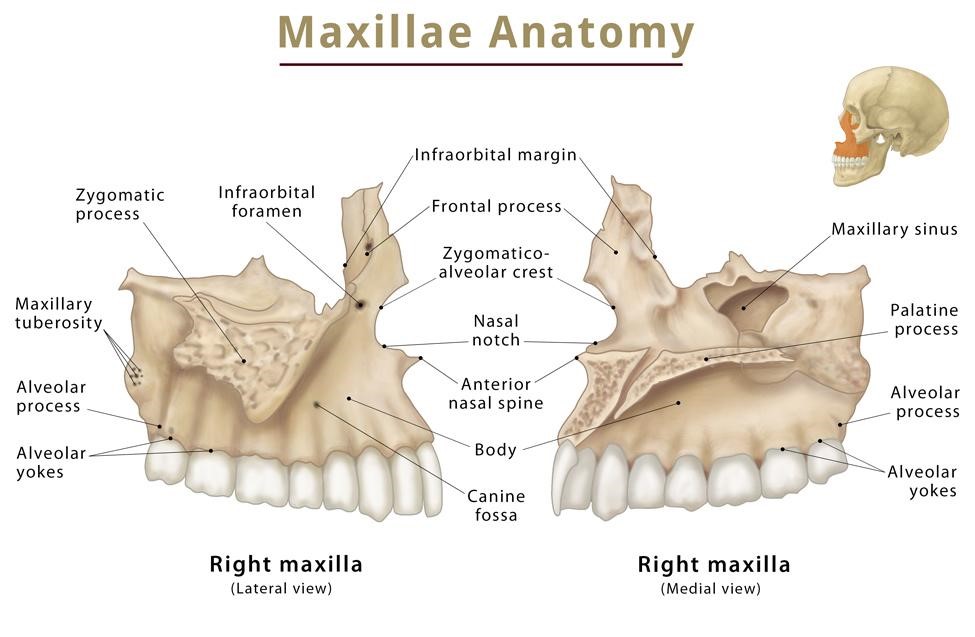
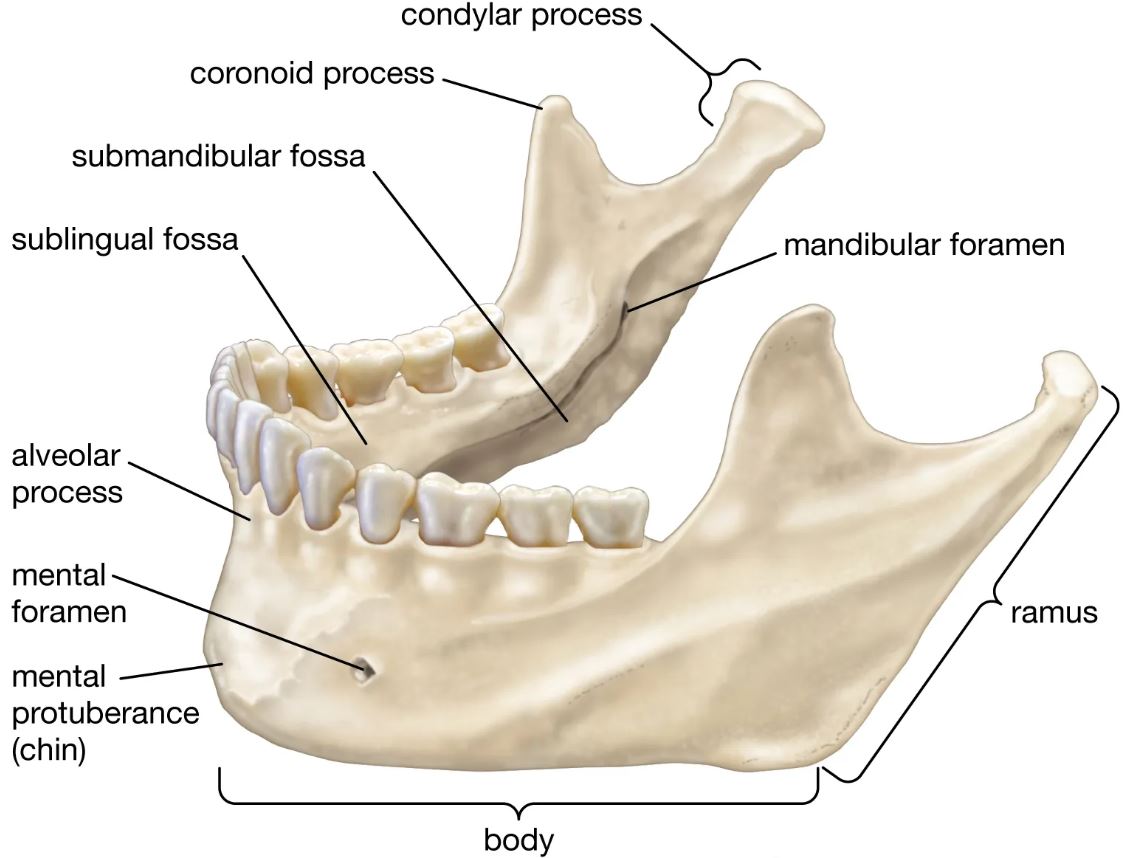
Local or generalized infection (osteomyelitis) and destruction/death (osteoradionecrosis) of bone and bone marrow in the maxilla or mandible or both. The maxilla is the upper part of a pair of bones that form the base of most of the upper face, roof of the mouth, sides of the nasal cavity, and floor of the orbit, commonly referred to as the upper jaw. The mandible is the large bone forming the lower jaw.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Etiology
Chronic osteomyelitis, is usually caused by bacteria introduced by trauma or surgery, by direct extension from a nearby infection (commonly a diseased tooth), or via the blood stream. Osteoradionecrosis, is usually caused by radiation to head and neck tumors. Radiation damage leads to diminished blood supply and decreased ability of tissues to heal if injured. Risk factors for maxilla or mandible osteomyelitis or osteoradionecrosis include debilitating co-morbid diseases, radiation, cancer, and diabetes mellitus.
Signs & Symptoms
{kind=link}
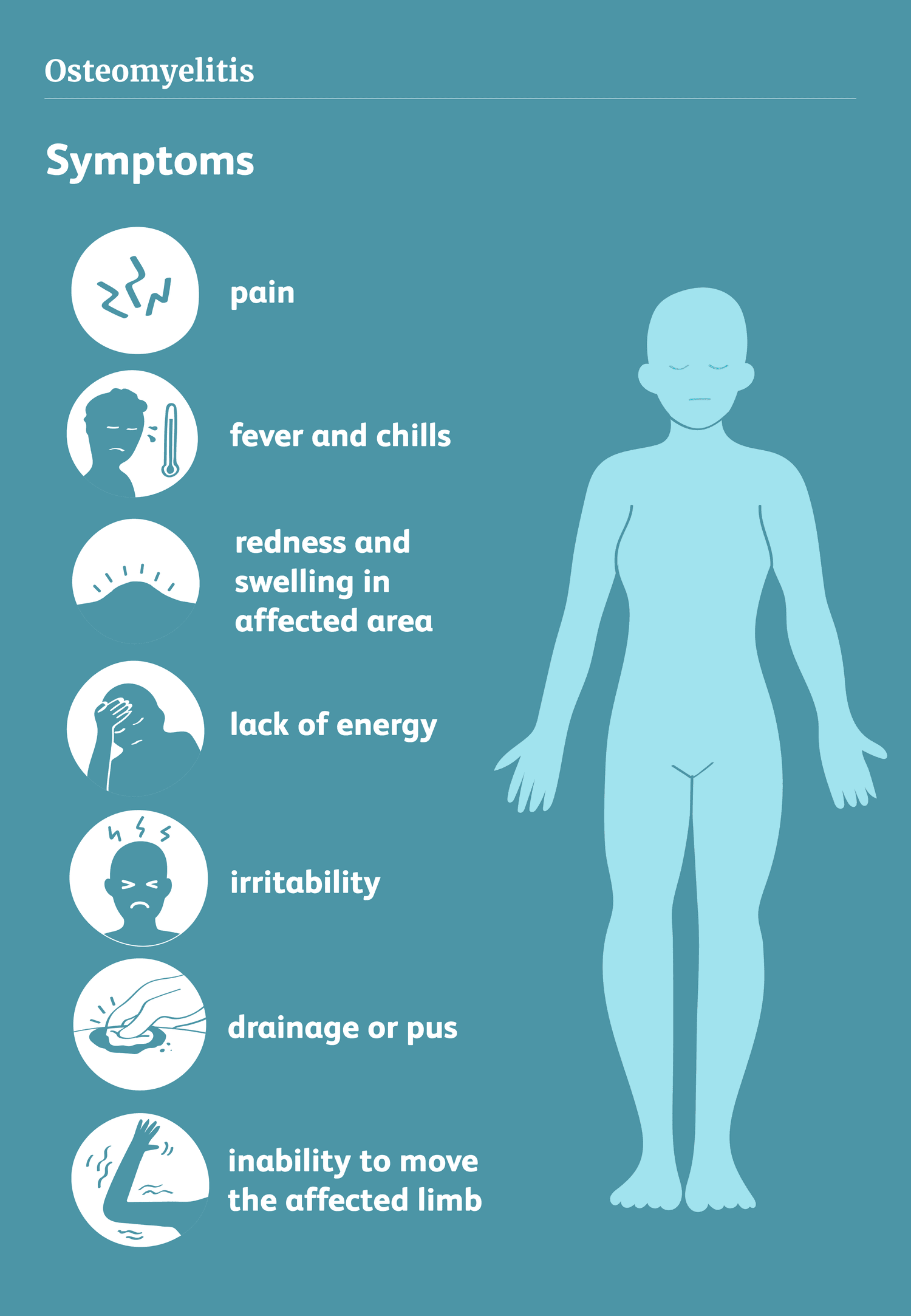
Persistent, severe, and increasing bone pain; localized warmth, swelling, erythema, and tenderness; sensory changes (numbness); guarding on movement; regional muscle spasm; weight loss; fatigue/ malaise; sweats; leukocytosis, and fever are the most often noted signs and symptoms.
Tests
Tests may include: white blood cell (WBC) count, erythrocyte sedimentation rate (ESR), x-rays (usually become abnormal after 3 to 4 weeks), computed tomography (CT) scan, bone biopsy, and culture and sensitivity tests of bone, tissue or pus.
{kind=link}
{kind=link}
Treatment
Parenteral (IV) antibiotics for 4 to 8 weeks, and surgery may be necessary to remove the necrotic or dead bone and tissue. Hyperbaric oxygen therapy (HBO), removal of necrotic bone and bone grafting may be necessary with both chronic osteomyelitis and osteoradionecrosis.
{kind=link}
Residuals
Both chronic osteomyelitis and osteoradionecrosis may persist for years causing prolonged pain and functional impairment. Treatment may require aggressive surgical management and both surgical and dental reconstruction.
Special Considerations
-
May be entitled to special monthly compensation where the Veteran has a single service-connected disability rated as 100% with additional service-connected disability or disabilities independently ratable at 60% or more, which are separate and distinct from the 100% service-connected disability and involves different anatomical segments or bodily systems. See 38 CFR 3.350(i)(1) – Special Monthly Compensation (SMC).
-
A report of the Institute of Medicine of the National Academy of Sciences has identified some long-term health effects, listed in the table embedded within 38 CFR 3.317(d), that potentially are associated with the infectious diseases listed in 38 CFR 3.317(c)(2). These health effects and diseases are listed alphabetically and are not categorized by the level of association stated in the National Academy of Sciences report. If a veteran who has or had an infectious disease identified in column A also has a condition identified in column B as potentially related to that infectious disease, VA must determine, based on the evidence in each case, whether the column B condition was caused by the infectious disease for purposes of paying disability compensation. This does not preclude a finding that other manifestations of disability or secondary conditions were caused by an infectious disease. See 38 CFR 3.317(d) - Long-term health effects potentially associated with infectious diseases.
-
If a veteran presumed service connected for one of the diseases listed in 38 CFR 3.317(c)(2) is diagnosed with one of the diseases listed in column “B” in the table embedded within 38 CFR 3.317(d) within the time period specified for the disease in the same table, if a time period is specified or, otherwise, at any time, VA will request a medical opinion as to whether it is at least as likely as not that the condition was caused by the veteran having had the associated disease in column “A” in that same table. See 38 CFR 3.317(d) - Long-term health effects potentially associated with infectious diseases.
-
Chronic, or recurring, suppural.;,tive osteomyelitis, once clinically identified, including chronic inflammation of bone marrow, cortex, or periosteum, should be considered as a continuously disabling process, whether or not an actively discharging sinus or other obvious evidence of infection is manifest from time to time, and unless the focus is entirely removed by amputation will entitle to a permanent rating to be combined with other ratings for residual conditions, however, not exceeding amputation ratings at the site of election.
Notes
-
For VA compensation purposes, diagnostic imaging studies include, but are not limited to, conventional radiography (X-ray), computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET), radionuclide bone scanning, or ultrasonography
-
Separately evaluate loss of vocal articulation, loss of smell, loss of taste, neurological impairment, respiratory dysfunction, and other impairments under the appropriate diagnostic code and combine under 38 CFR 4.25 for each separately rated condition.
-
A rating of 10 percent, as an exception to the amputation rule, is to be assigned in any case of active osteomyelitis where the amputation rating for the affected part is no percent. This 10 percent rating and the other partial ratings of 30 percent or less are to be combined with ratings for ankylosis, limited motion, nonunion or malunion, shortening, etc., subject, of course, to the amputation rule. The 60 percent rating, as it is based on constitutional symptoms, is not subject to the amputation rule. A rating for osteomyelitis will not be applied following cure by removal or radical resection of the affected bone.
-
The 20 percent rating on the basis of activity within the past 5 years is not assignable following the initial infection of active osteomyelitis with no subsequent reactivation. The prerequisite for this historical rating is an established recurrent osteomyelitis. To qualify for the 10 percent rating, 2 or more episodes following the initial infection are required. This 20 percent rating or the 10 percent rating, when applicable, will be assigned once only to cover disability at all sites of previously active infection with a future ending date in the case of the 20 percent rating.