7101 - Hypertensive vascular disease (hypertension and isolated systolic hypertension)
DBQ: Link to Index of DBQ/Exams by Disability for DC 7101
Acronym: HCVD
Definition
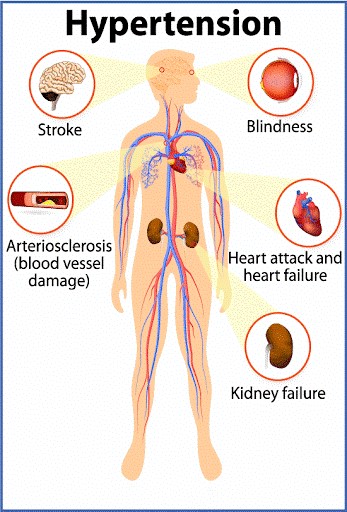
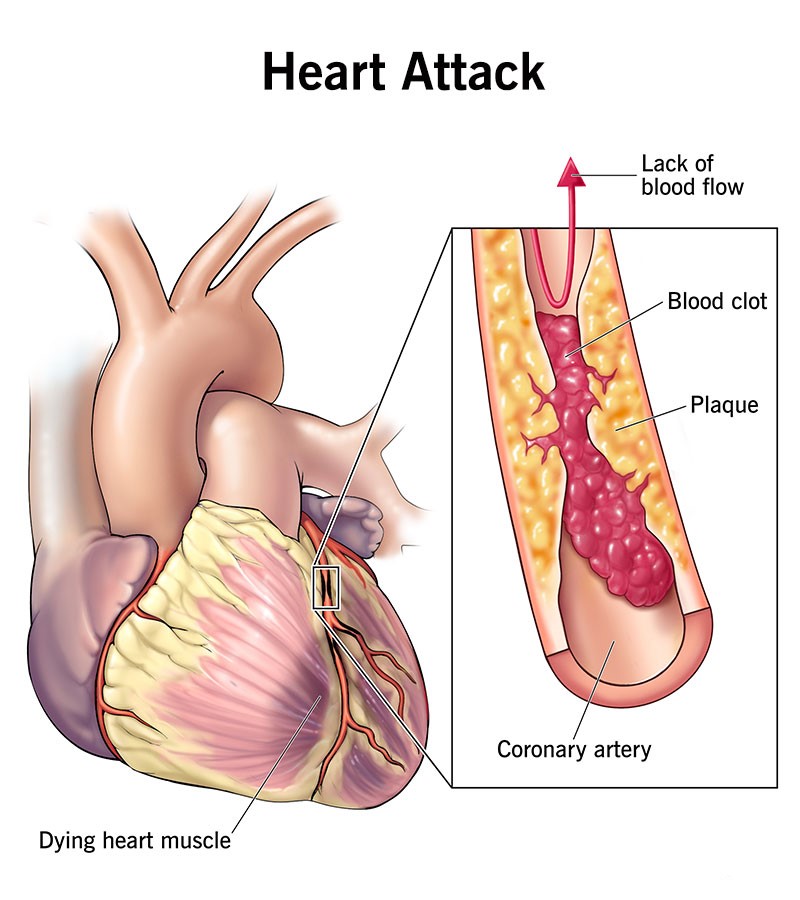
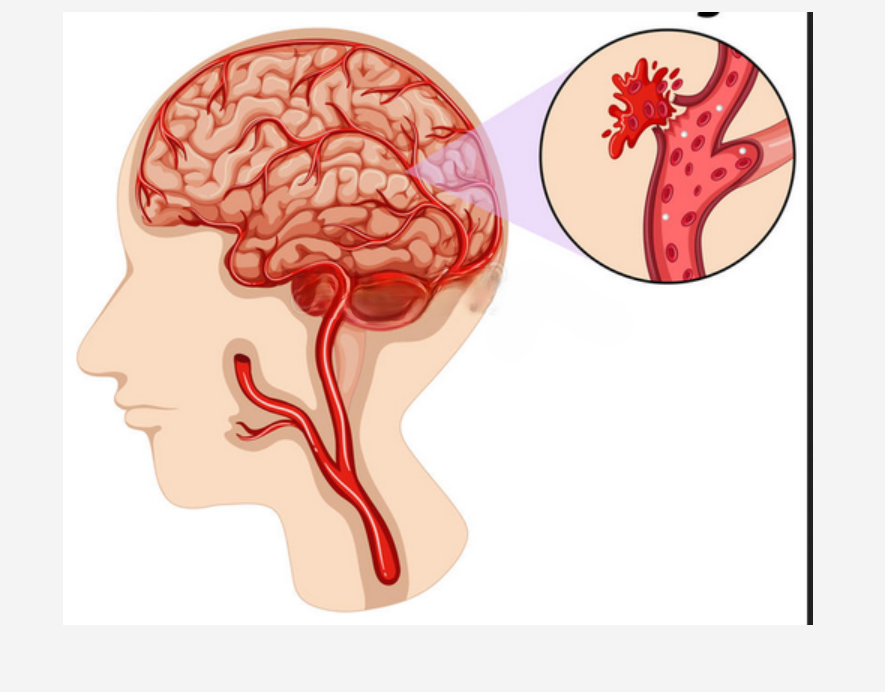
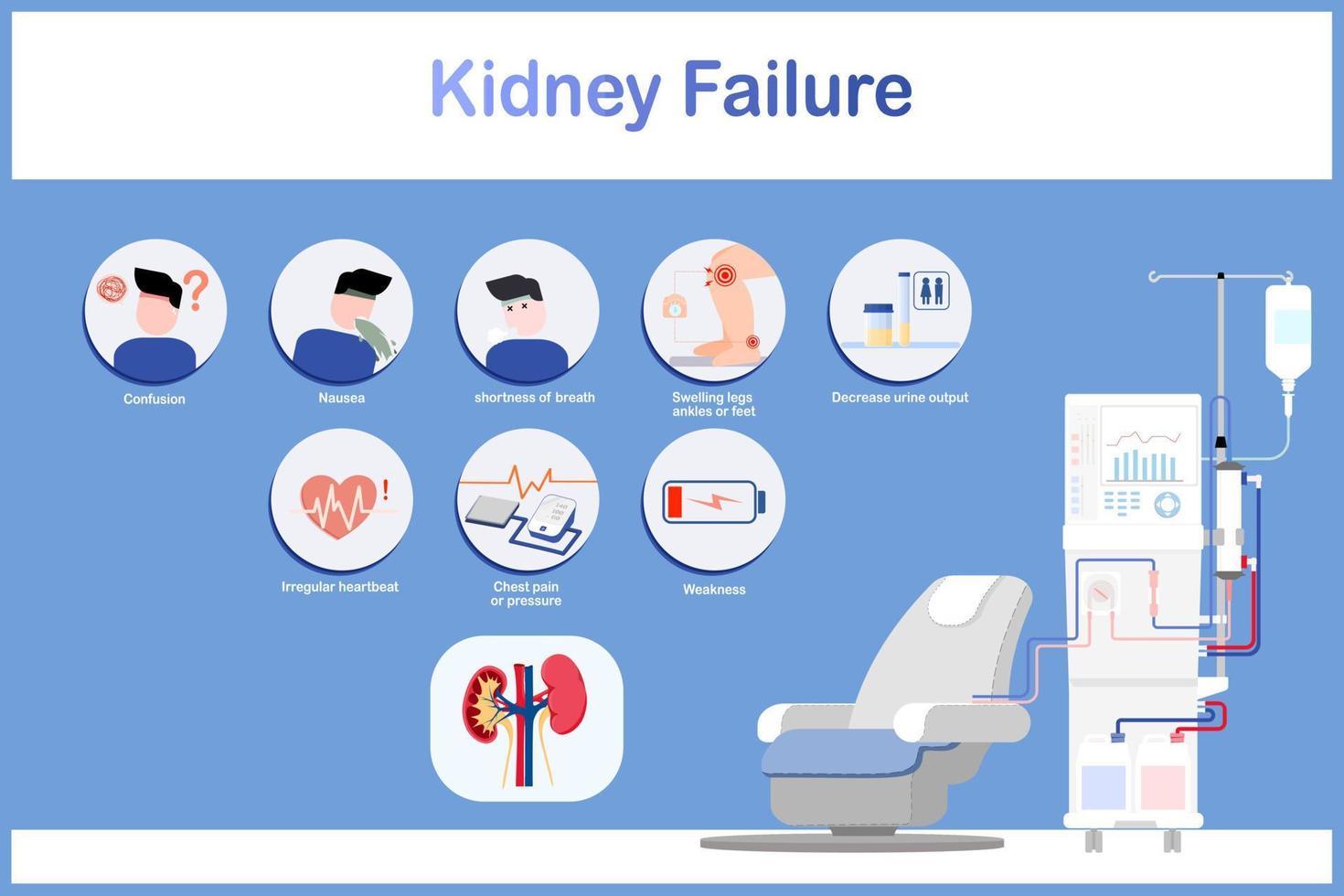
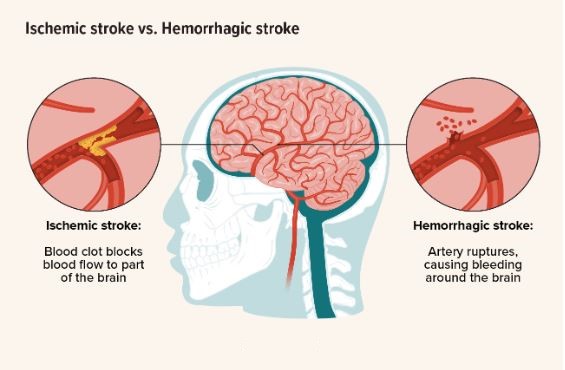
Untreated and long-standing hypertension can lead to hypertensive vascular disease, which affect the blood vessels through the build-up of atherosclerotic plaque. Portions of this plaque can break off and lodge in blood vessels causing heart attacks, strokes, and kidney failure.
Hypertension in persons over 18 years of age is defined by blood pressure readings of a diastolic average, taken on two separate occasions, as over 90 mm/Hg, or systolic average, at two or more visits, which is over 140 mm/Hg.
Normal blood pressure should be 120/80 mm/Hg or lower. Prehypertension blood pressure is a systolic pressure of 120-130 mm/Hg and a diastolic pressure of 80-90 mm/Hg. Stage I hypertension is a systolic pressure of 140-159 mm/Hg or a diastolic pressure of 90-99 mm/Hg. Stage II hypertension is systolic pressure of 160 mm/Hg or higher or a diastolic pressure 100 mm/Hg or higher. Diagnosis is made through two seated blood pressure readings on two separate occasions.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Etiology
The etiology in primary hypertension is unknown in 90 to 95% of cases. Heredity may be a factor, as well as race (more common in blacks), tobacco usage, use of oral contraceptives, and a sedentary old age. Genetically, susceptible people react to some of the disease-related environmental factors, such as, diet, salt, stress, and obesity with hypertension.
Secondary hypertension is caused by an underlying condition and often appears suddenly. Various medications and conditions can lead to secondary hypertension. Some causes are:
-
Kidney disease
-
Tumors of the adrenal gland
-
Certain congenital heart defects such as coarctation of the aorta
-
Certain medications such as birth control pills, cold remedies, decongestants, over-the-counter pain relievers
-
Certain disease states, such as, pheochromocytoma, Cushing's syndrome, and dysfunction of the parathyroid, pituitary or thyroid glands.
Signs & Symptoms
The characteristic manifestations are consistent high blood pressure measurements. Some patient complaints related to high blood pressure may be headache upon awakening that later subsides, dizziness, fatigue and impotence. There may also be blurring of vision, nosebleeds, and shortness of breath. When vascular changes have taken place from long-term hypertension, the target organs and problems are as follows: heart, with coronary artery disease; kidneys, with renal failure; eyes, with retinal disorders; peripheral vascular system, with claudication and thrombosis; and cerebrovascular system, with transient ischemic attacks (TIA) and stroke (CVA).
{kind=link}
Tests
Basic studies recommended for patients with hypertension include history and physical examination. In addition, the following laboratory studies are parts of the diagnostic assessment:
-
Complete blood count (CBC)
-
Serum studies of potassium, sodium, glucose, blood urea nitrogen (BUN), Cholesterol, lipids, and creatinine
-
Chest x-ray and screening for secondary causes of hypertension may be indicated.
{kind=link}
{kind=link}
{kind=link}
Treatment
Lifestyle changes and drug therapy can control primary hypertension. The general goal is to lower the diastolic pressure below 80 mm/Hg, and to keep the systolic pressure 120 or below mm/Hg with a minimum of adverse effects from medication. Exercise, weight loss, restriction of salt and saturated fat, use of relaxation techniques, and cessation of smoking are all considered to be beneficial in blood pressure reduction
Residuals
Patients with hypertension are advised to avoid over-the-counter cold and sinus medications because the vasoconstrictors that they contain would be harmful to them. A patient's age, race, and medical condition will influence the selection of antihypertensive medication. Sexual dysfunction is one side effect of many of these medications. Some drugs increase cholesterol levels, aggravate diabetes mellitus in susceptible patients, bring about symptoms of gout, or cause sleep disturbances. These reactions to the therapy make compliance difficult. Patients who are non-compliant with treatment as well as untreated hypertensive patients are at risk of developing disabling or fatal left ventricular heart failure, myocardial infarction (MI), brain hemorrhage or infarction (CVA), or renal failure at an early age.
{kind=link}
{kind=link}
Special Considerations
-
If the Veteran is a former prisoner of war and was interned or detained for not less that 30 days, this disease shall be service connected if manifest to a degree of disability of 10 percent or more at any time after discharge or release from active military, naval, or air service even though there is no record of such disease during service, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied [38 CFR 3.309 (c) Disease subject to presumptive service connection].
-
Obstructive sleep apnea is a cause/risk factor for hypertension. Referral for a polysomnography (sleep study) can identify this disorder. Patients with drug-resistent hypertension and a history of snoring should be evaluated for obstructive sleep apnea. Treatment for this disorder is through use of continuous positive airway pressure (CPAP) administered during sleep to maintain an open airway and improve oxygenation of the blood.
-
Separate ratings are not to be assigned for disability from disease of the heart and any form of nephritis, on account of the close interrelationships of cardiovascular disabilities. If, however, absence of a kidney is the sole renal disability, even if removal was required because of nephritis, the absent kidney and any hypertension or heart disease will be separately rated. Also, in the event that chronic renal disease has progressed to the point where regular dialysis is required, any coexisting hypertension or heart disease will be separately rated. [38 CFR 4.115 – Nephritis]
-
Certain arteriosclerotic manifestations diagnosed in a Veteran who presents a service-connected hypertension will be service connected through his/her relationship to the hypertension.
-
If a Veteran is a former prisoner of war, this disease shall be service connected if manifest to a degree of disability of 10% or more at any time after discharge or release from active military, naval, or air service even though there is no record of such disease during service, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied [38 CFR 3.309 (c) Disease subject to presumptive service connection], 38 CFR 3.309(a) [chronic disease], 38 CFR 3.309(e). Disease subject to presumptive service connection.
-
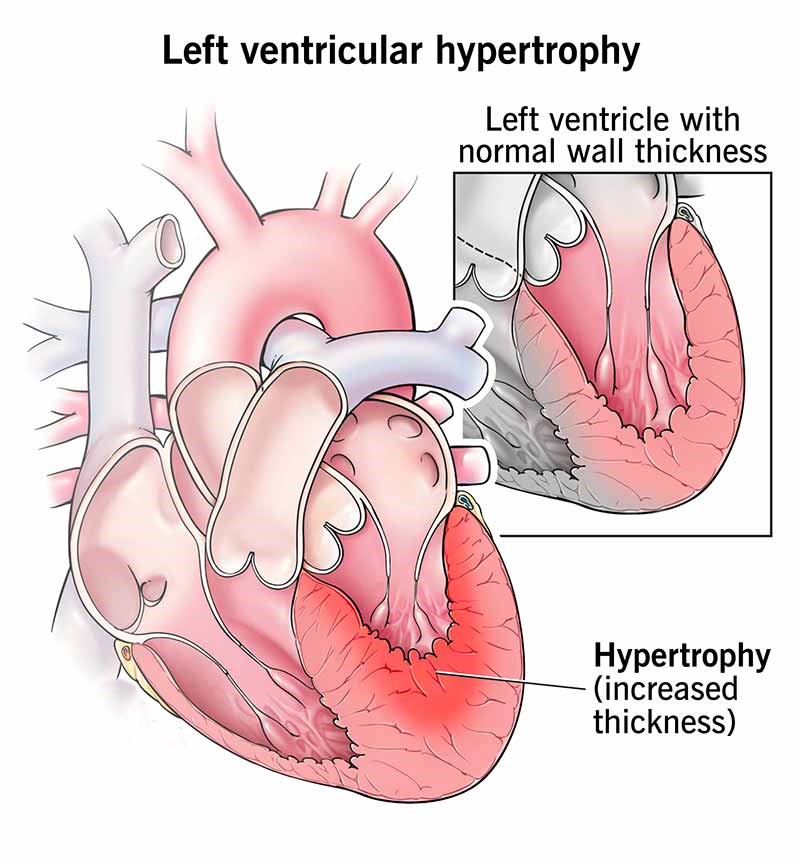
Hypertensive Vascular Disease - The cause of hypertension is unknown in the vast majority of cases. Do not rate elevation of systolic blood pressure due to aortic insufficiency or thyrotoxicosis and elevation of systolic or diastolic blood pressure due to nephritis separately from the primary disease. Hypertension may exist for years without causing symptoms. On the other hand, if sufficiently severe, it may so increase the cardiac load as to result in hypertrophy of the cardiac muscle or in cardiac dilation and decompensation.
-
If the hypertension is long continued, there may occur an arteriosclerosis of uneven distribution which often involves the vessels of one organ to a greater degree than those of the rest of the body. If it is of sufficient degree to cause significant impairment of the circulation to the organ, it will cause symptoms in accordance with the organ involved and with the degree of impairment. In the brain it may cause symptoms and signs warranting a diagnosis of cerebral arteriosclerosis or thrombosis with hemiplegia. Nephrosclerosis may occur with impairment of renal function. In the heart myocardial damage or coronary occlusion may result. But, it should be kept in mind that arteriosclerosis occurs with advancing age without a preexisting hypertension, and it may occur in some younger individuals who are predisposed to arterial changes. The existence of an arteriosclerosis does not therefore imply or indicate a previous hypertension.
-
If any of the above arteriosclerotic manifestations are diagnosed in a veteran who presents a service-connected hypertension, hold him/her to be service connected through his/her relationship to the hypertension.
-
Obstructive sleep apnea is risk factor for hypertension. Referral for a polysomnography (sleep study) can identify this disorder. Patients with drug-resistant hypertension and a history of snoring should be evaluated for obstructive sleep apnea. Treatment for this disorder is through use of continuous positive airway pressure administered during sleep to maintain an open airway and improve oxygenation of the blood.
-
Notes
-
Hypertension or isolated systolic hypertension must be confirmed by readings taken two or more times on at least three different days. For purposes of this section, the term hypertension means that the diastolic blood pressure is predominantly 90mm. or greater, and isolated systolic hypertension means that the systolic blood pressure is predominantly 160mm. or greater with a diastolic blood pressure of less than 90mm
-
Evaluate hypertension due to aortic insufficiency or hyperthyroidism, which is usually the isolated systolic type, as part of the condition causing it rather than by a separate evaluation.
-
Evaluate hypertension separately from hypertensive heart disease and other types of heart disease.
-
The rating criteria for cardiovascular conditions underwent full-scale revision effective on November 14, 2021 and January 12, 1999. A regulatory change was effective August 13, 1998, updated criteria for cold injury residuals under 38 CFR 4.104, DC 7122. The changes are not considered liberalizing and should not be used as the basis for reduction unless the disability has actually improved.