7000 - Valvular heart disease (including rheumatic heart disease)
Alternate Code: Aortic stenosis
DBQ: Link to Index of DBQ/Exams by Disability for DC 7000
Acronym: VHD
Definition
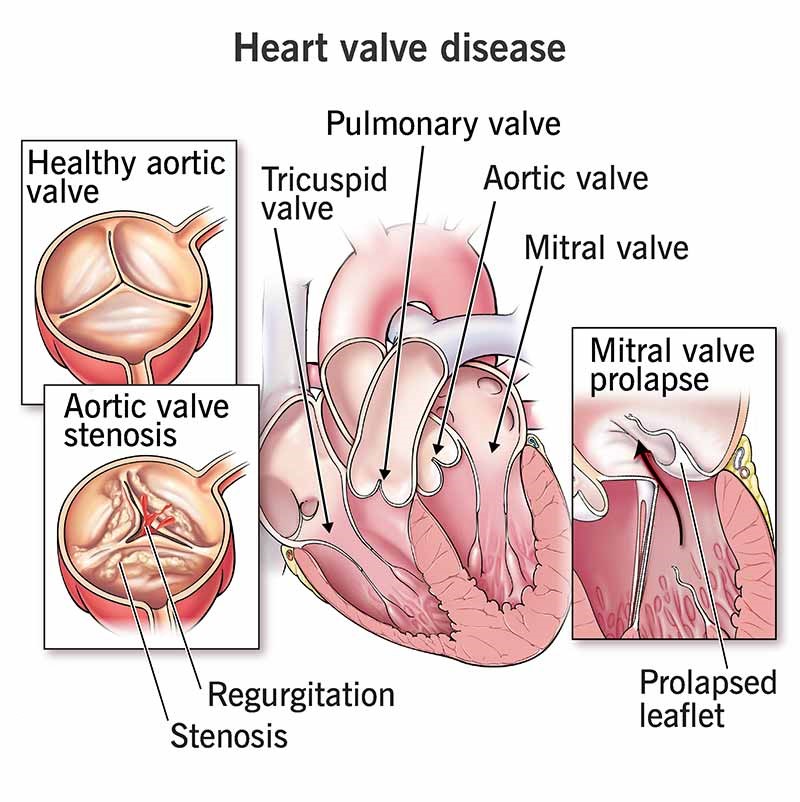
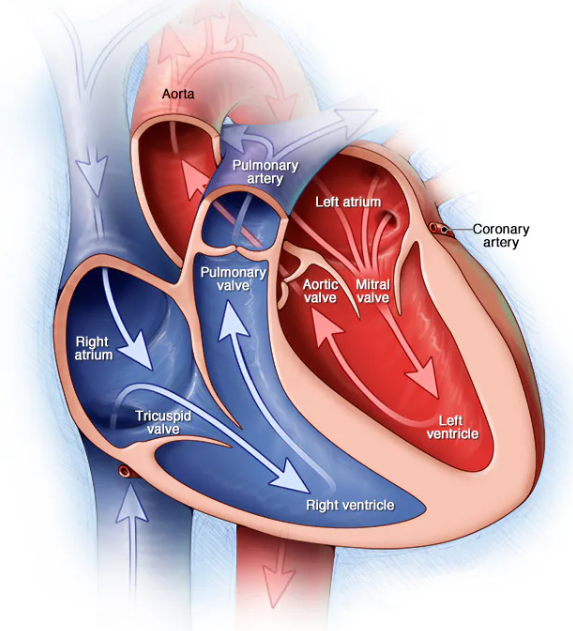
Valvular heart disease refers to conditions affecting any of the four valves of the heart; mitral, aortic, pulmonary, or tricuspid. The condition prevents efficient blood flow through the heart. Valvular heart disease includes: valvular tissue thickening that narrows the valvular opening, and valvular problems that prevent complete valve closure of any of the four valves, resulting in leakage of the valve. Specific definitions of conditions affecting the heart valves are as follows:
{kind=link}
-
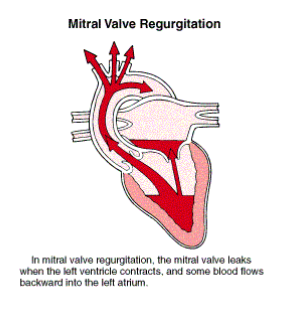
Mitral insufficiency/regurgitation - A condition in which there is a backward flow from the left ventricle through a malfunctioning mitral valve into the left atrium.
-
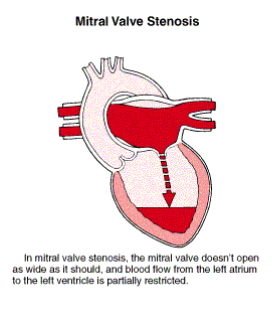
Mitral Stenosis - A condition in which flow from the left atrium to the left ventricle is obstructed because of a narrowing of the mitral opening.
-
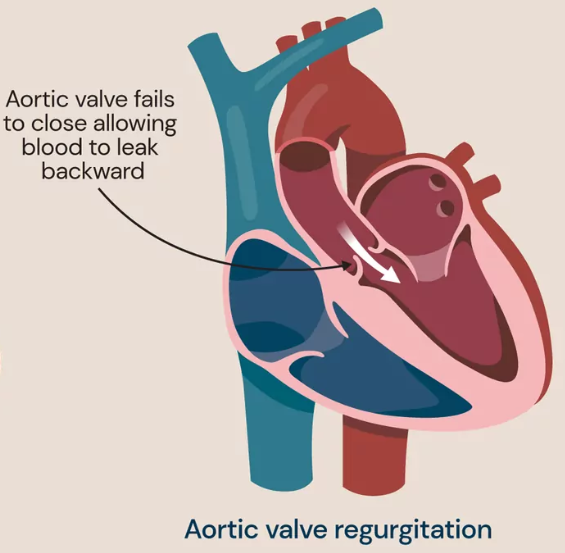
Aortic Insufficiency/regurgitation - A condition in which there is a backwards flow from the aorta into the left ventricle through malfunctioning aortic cusps or the aortic semilunar valve (valve between left ventricle and aorta). (A discussion of rheumatic heart disease follows the entry for valvular heart disease.)
{kind=link}
{kind=link}
{kind=link}
Etiology
The causes of valvular heart diseases vary according to the involved valve, and also to whether or not the disease is related to stenosis or insufficiency. Almost all of the valvular heart diseases are associated with rheumatic fever. Causes of specific conditions of the heart valves are as follows:
-
Mitral insufficiency may be caused by rheumatic fever, hypertension, endocarditis, infection, subaortic stenosis, mitral valve prolapse, myocardial infarction (MI), severe left ventricular failure, or ruptured chordae tendineae. The condition may also be associated with congenital anomalies. The most common cause of mitral stenosis is rheumatic fever.
-
Aortic Insufficiency may be caused by rheumatic fever, syphilis, hypertension, and endocarditis. It may be idiopathic, and also associated with Marfan's syndrome and ventricular septal defect, even after the defect has been closed surgically. Aortic stenosis may be caused by congenital stenosis of the aortic bicuspid valve, congenital stenosis of valve cusps, and rheumatic fever, or due to calcification of the valve.
-
Pulmonary insufficiency may result from pulmonary hypertension; however, the condition may be congenital. In rare instances, it may result from prolonged use of a pressure-monitoring catheter. Pulmonary stenosis may result in congenital stenosis of the valve cusps and, occasionally, it may result from rheumatic fever. The condition has also been associated with congenital heart defects.
-
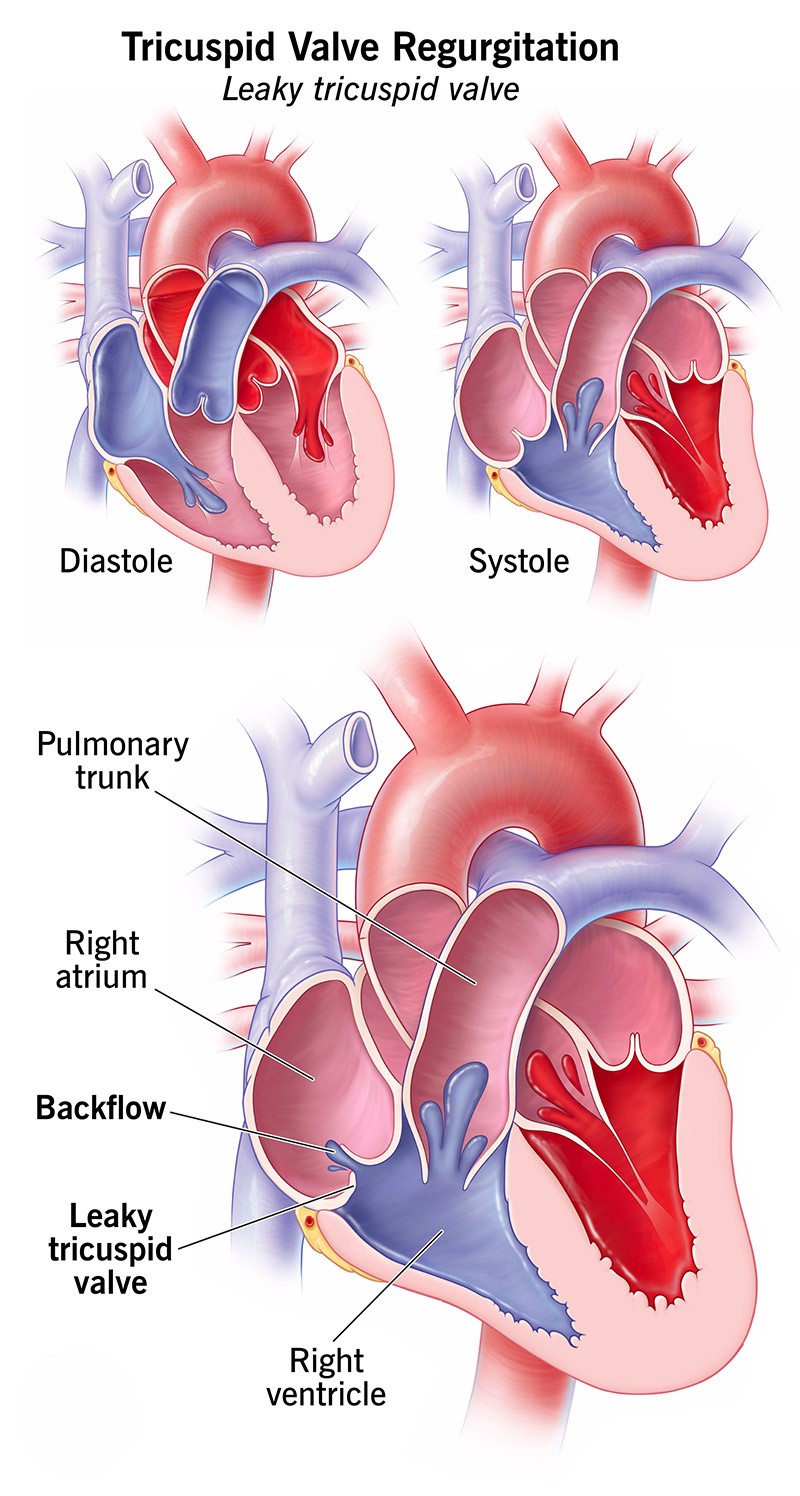
Tricuspid insufficiency (tricuspid regurgitation or incompetence) may be caused by right ventricular failure, rheumatic fever, endocarditis, pulmonary hypertension, pulmonary emboli, or a permanent placement pacing catheter. It is rarely caused by trauma endocarditis. Tricuspid stenosis may result from rheumatic fever. It has also been related to mitral or aortic valvular disease.
{kind=link}
{kind=link}
Signs & Symptoms
The signs and symptoms will vary with the valve affected. Manifestations of conditions related to each of the following valve diseases are as follows:
-
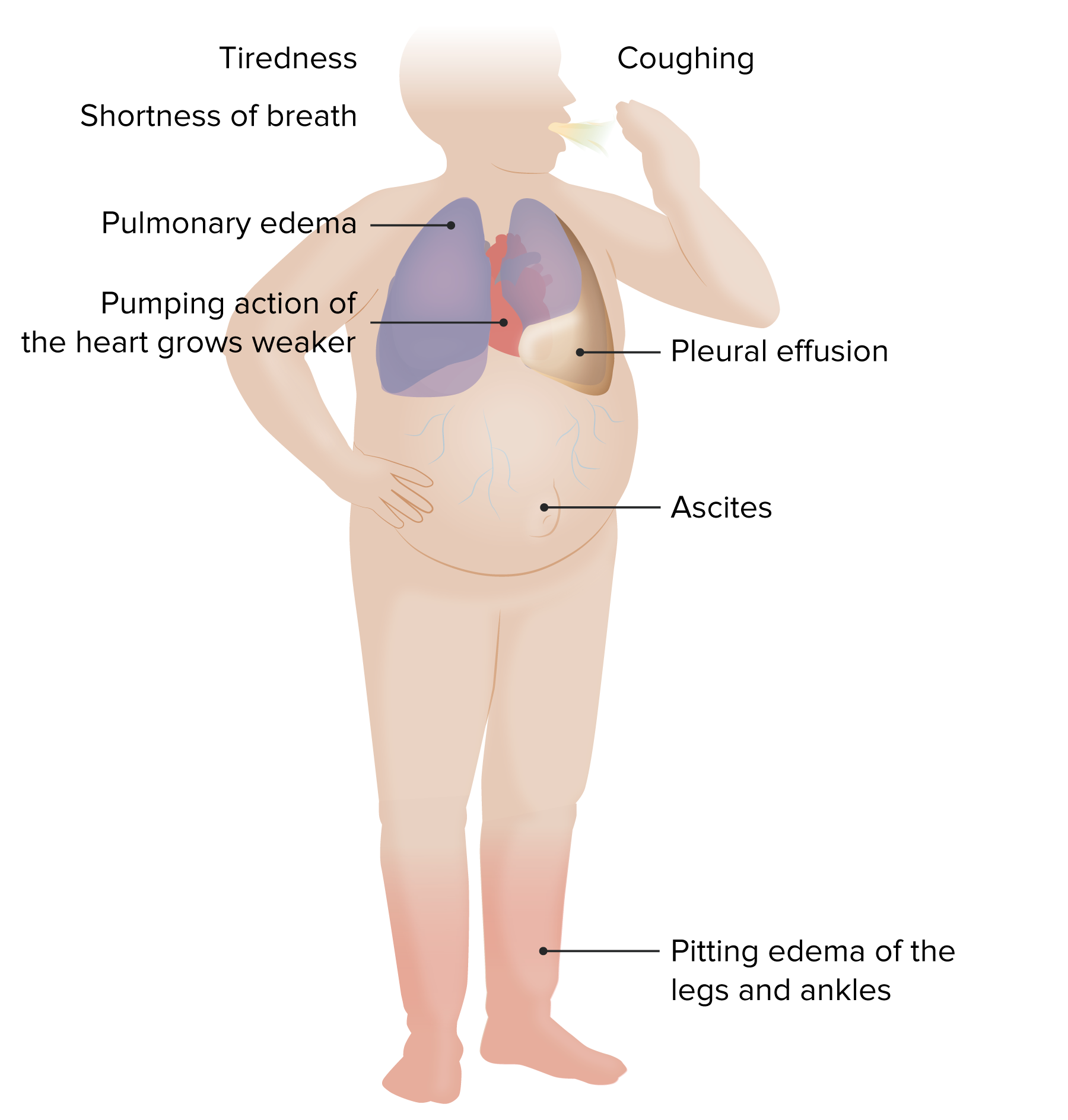
Mitral valve disease - Signs and symptoms may include: orthopnea; and dyspnea; pulmonary edema. In mitral insufficiency, there is also a holosystolic murmur; angina; palpitations; peripheral edema; jugular vein distention; hepatomegaly from right ventricular failure; tachycardia and crackles in the lungs. Additional signs and symptoms for mitral stenosis include: paroxysmal, nocturnal dyspnea, hemoptysis, ascites, hepatomegaly, cardiac dysrhythmias, systemic emboli, and a diastolic murmur at the apex of the heart.
-
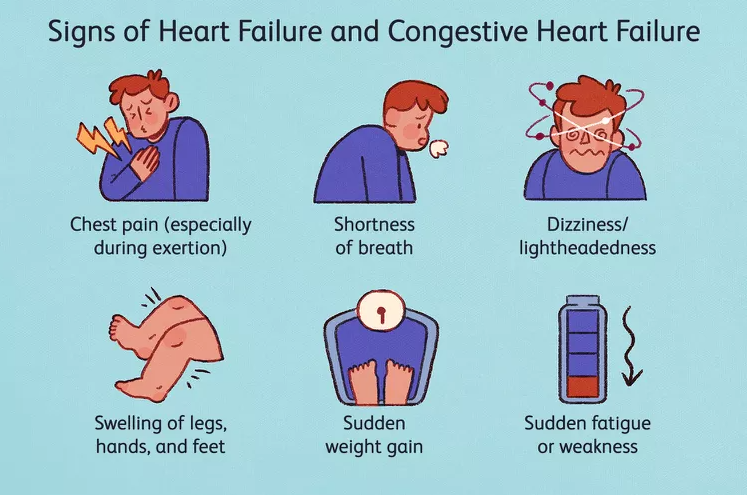
Aortic valve disease Signs and symptoms may include: dyspnea; cough; fatigue; palpitations; angina; syncope; pulmonary vein congestion; congestive heart failure (CHF); pulmonary edema; Quincke's sign; rapidly rising and collapsing pulses; cardiac dysrhythmias; and systemic emboli. Additional signs and symptoms of aortic insufficiency include: diminished carotid pulses, decreased cardiac output, possible pulsus alternans, and a diastolic blowing murmur at the left sternal border. In aortic stenosis, there is a systolic murmur at the base that may radiate to the carotids and arteries in the neck.
-
Pulmonary valve disease - Signs and symptoms include those identified for stenosis and insufficiency as noted above. A diastolic murmur in the pulmonary area for pulmonary insufficiency is also included. In pulmonary stenosis, there is a systolic murmur at the left sternal border and a split accentuated (S2).
-
Tricuspid valve disease - Signs and symptoms are the same as noted above. Also included are a possible S3 and systolic murmur at the lower left sternal border that increases with inspiration, and a diastolic murmur at the lower left sternal border that increases with inspiration.
{kind=link}
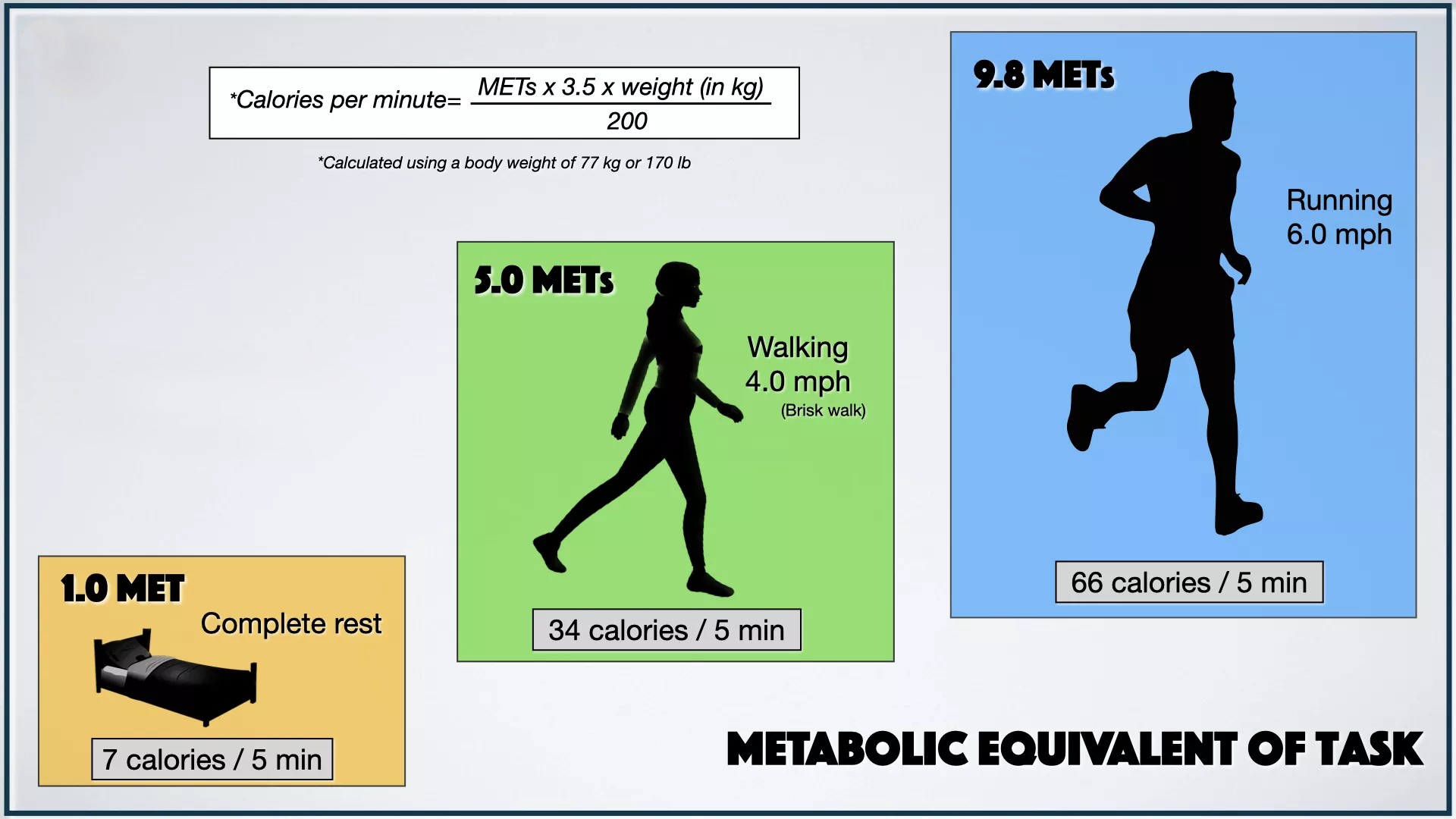
The functional abilities of cardiac patients can be classified in terms of metabolic equivalents (METs). The classification is generally as follows:
{kind=link}
-
Light to medium housework is 2 to 4 METs
-
Heavy housework or yard work is approximately 5 to 6 METs
-
Strenuous activity would be 7 to 10 METs, etc.
To determine the limitations on patient's functional abilities, the METs are considered in accordance with what symptoms are exhibited when the activities are carried out. For example, if a patient is performing activity at the 2 to 4 MET level and experiences dyspnea, fatigue, dizziness or fainting, the patient is considered to have low functional abilities.
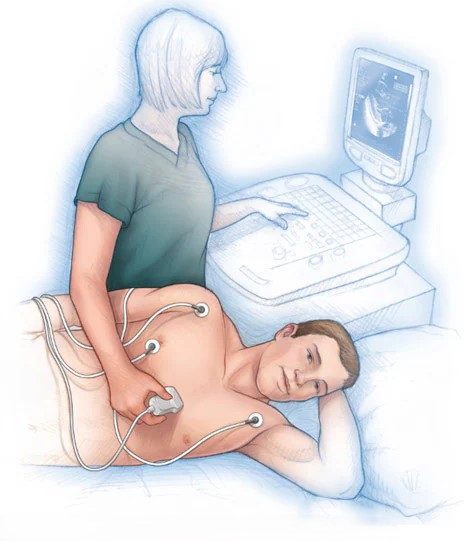
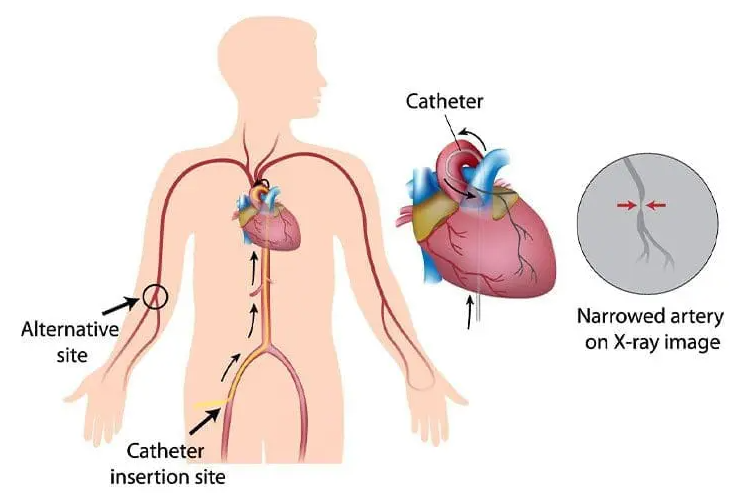
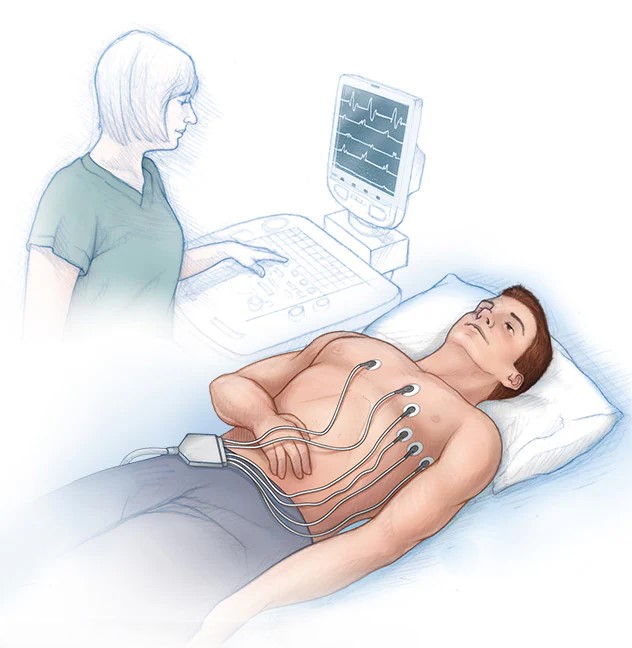
Tests
Tests for the conditions may include: physical examination, 2D echocardiogram with Doppler, cardiac catheterization, x-rays, and electrocardiogram (EKG).
{kind=link}
{kind=link}
{kind=link}
Treatment
The treatment of valvular heart disease depends on the valve involved and the nature and the severity of the symptoms. The treatment includes drug therapy that includes beta- blockers, anticoagulants, and antibiotics; and a sodium-restricted diet. Open-heart surgery may also be indicated to replace damaged valves.
Residuals
The residual varies with the specific valvular heart disease. Reduced or restricted activities are needed in aortic stenosis to avoid sudden death on exertion. Recurrent CHF is possible. Continued monitoring is needed for pulmonary edema or heart failure because of severe valvular heart disease.
Special Considerations
-
May be entitled to special monthly compensation where the Veteran has a single service-connected disability rated as 100% with additional service-connected disability or disabilities independently ratable at 60% or more, which are separate and distinct from the 100% service-connected disability and involves different anatomical segments or bodily systems. See 38 CFR 3.350(i)(1) – Special Monthly Compensation (SMC).
-
Rheumatic Heart Disease. Chronic rheumatic heart disease results from a single or repeated attacks of rheumatic fever which produce rigidity and deformity of the cusps, fusion of the commissures, or shortening and fusion of the chordae tendineae. The earliest evidence of organic valvular disease is a significant murmur. The earliest evidence of hemodynamically significant valvular lesions is found on x-ray, fluoroscopy, and ECG study, since these will reveal the earliest stages of specific chamber enlargement. With a history of rheumatic fever in service, an aortic valve insufficiency that manifests some years later without other cause shown will be service connected.
-
Coexisting forms of heart disease. Accepted medical principles do not concede an etiological relationship between rheumatic heart disease and either hypertensive or arteriosclerotic heart disease.
-
Rheumatic Heart Disease and Hypertensive or Arteriosclerotic Changes - If a Veteran who is service connected for rheumatic heart disease develops hypertensive or arteriosclerotic heart disease after the applicable presumptive period following military discharge, request a medical opinion to determine which condition is causing the current signs and symptoms. If the examiner is unable to separate the effects of one type of heart disease from another, they must be rated together. Since medically there is no recognized etiological relationship between rheumatic heart disease and later developing hypertensive or arteriosclerotic changes, do not extend service connection to systemic manifestations or arteriosclerosis in areas remote from the heart.
-
This disease shall be granted service connection although not otherwise established as incurred in or aggravated by service if manifested to a compensable degree within the applicable time limits under 38 CFR 3.307 following service in a period of war or following peacetime service on or after January 1, 1947, provided the rebuttable presumption provisions of 38 CFR 3.307 are also satisfied [38 CFR 38 CFR 3.309 . [Disease subject to presumptive service connection], 38 CFR 3.309 (a) [chronic disease].
-
Grant SC on a secondary basis for the following conditions that develop subsequent to the service-connected (SC) amputation of one lower extremity at or above the knee, or SC amputations of both lower extremities at or above the ankles: IHD, or other cardiovascular disease, including hypertension.
Notes
-
Absent instructions otherwise in individual diagnostic codes, if there are cardiovascular and comorbid respiratory conditions that can be evaluated by Metabolic Equivalents (METs), only the disability from one body system may be evaluated using METs, while the disability involving the other body system must be evaluated by criteria other than METs.
-
One MET (metabolic equivalent) is the energy cost of standing quietly at rest and represents an oxygen uptake of 3.5 milliliters per kilogram of body weight per minute. When the level of METs at which breathlessness, fatigue, angina, dizziness, or syncope develops is required for evaluation, and a laboratory determination of METs by exercise testing cannot be done for medical reasons, a medical examiner may estimate the level of activity (expressed in METs and supported by specific examples, such as slow stair climbing or shoveling snow) that results in those symptoms.
-
For this general formula, heart failure symptoms include, but are not limited to, breathlessness, fatigue, angina, dizziness, arrhythmia, palpitations, or syncope.
-
The rating criteria for cardiovascular conditions underwent full-scale revision effective on November 14, 2021 and January 12, 1999. A regulatory change was effective August 13, 1998, updated criteria for cold injury residuals under 38 CFR 4.104, DC 7122. The changes are not considered liberalizing and should not be used as the basis for reduction unless the disability has actually improved.
{kind=link}